Case Western Reserve University School of Medicine, Cleveland, OH, USA.
J Cyst Fibros. 2011 Dec;10(6):453-9. doi: 10.1016/j.jcf.2011.07.003. Epub 2011 Jul 30.
Reduction in pulmonary exacerbations is an important efficacy endpoint for CF clinical studies. Powering exacerbation endpoints requires estimation of the future exacerbation incidence in CF study populations, but rates differ across the population.
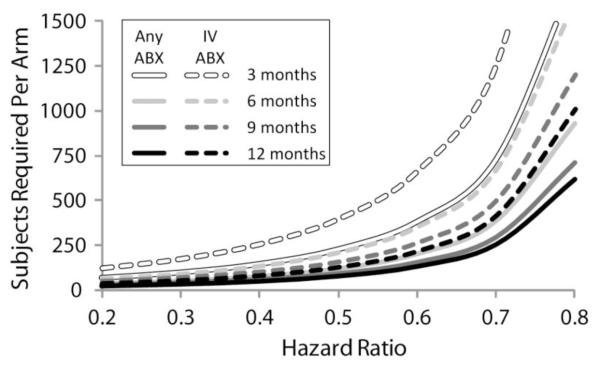
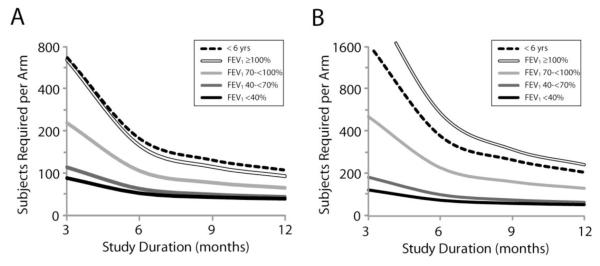
We have estimated exacerbation rates for Epidemiologic Study of CF subpopulations stratified by age, FEV(1)% predicted, sex, weight-for-age percentile, respiratory signs and symptoms, and history of exacerbation and bacterial culture. Sample sizes required to attain 80% power to detect exacerbation reductions of 20% to 80% in 1:1 randomized studies of 3 to 12 month duration were determined. Exacerbation treatments with "any" antibiotic (new oral quinolone, new inhaled antibiotic, or intravenous (IV) antibiotic) and with IV antibiotics were studied.
At all ages, decreased FEV(1), female sex, exacerbation history, and Pseudomonas aeruginosa culture history were associated with increased treatment for exacerbation.
These data should assist investigators in the design of future CF exacerbation studies.
减少肺部恶化是 CF 临床研究的一个重要疗效终点。为了使恶化终点具有说服力,需要对 CF 研究人群中的未来恶化发生率进行估计,但在人群中发生率有所不同。
我们根据年龄、FEV1%预计值、性别、体重-年龄百分位、呼吸体征和症状以及恶化和细菌培养史,对 CF 亚人群进行分层,估计恶化率。为了在 3 至 12 个月的 1:1 随机研究中检测到恶化减少 20%至 80%的 80%效力,确定了所需的样本量。研究了使用“任何”抗生素(新口服喹诺酮类药物、新吸入抗生素或静脉内(IV)抗生素)和 IV 抗生素治疗恶化的情况。
在所有年龄段,FEV1 下降、女性性别、恶化史和铜绿假单胞菌培养史与恶化的治疗增加有关。
这些数据应有助于研究人员设计未来的 CF 恶化研究。