Matouk Elias, Nguyen Dao, Benedetti Andrea, Bernier Joanie, Gruber James, Landry Jennifer, Rousseau Simon, Ahlgren Heather G, Lands Larry C, Wojewodka Gabriella, Radzioch Danuta
Adult Cystic Fibrosis Clinic, Montreal Chest Institute, McGill University, Canada; McGill University Health Center Research Institute, Canada; Department of Medicine, McGill University, Canada.
McGill University Health Center Research Institute, Canada; Department of Medicine, McGill University, Canada; Meakins-Christie Laboratories, Montreal Chest Institute, McGill University Health Centre, Canada.
J Pulm Respir Med. 2016 Oct 14;6(5):1000375. doi: 10.4172/2161-105X.1000375.
In stable adult cystic fibrosis (CF) patients, we assessed the role of baseline high sensitivity C-reactive protein (hs-CRP) on CF clinical variables and frequency of intravenous (IV) treated pulmonary exacerbations (PExs) 1-year post-baseline.
We recruited 51 clinically stable CF patients from our Adult CF Center. We incorporated collected parameters into Matouk CF clinical score and CF questionnaire-revised quality of life score (QOL). We used the clinical minus complications subscores as a clinical disease activity score (CDAS). We dichotomized our patients according to the cohort median baseline hs-CRP of 5.2 mg/L.
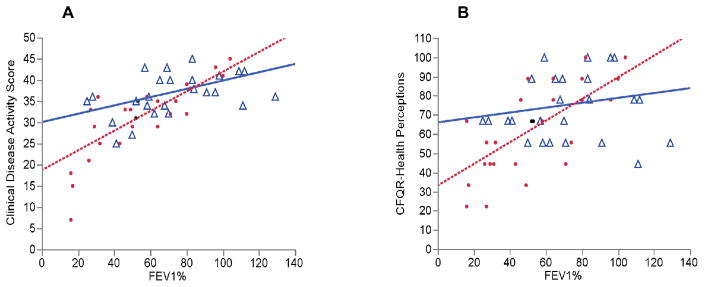
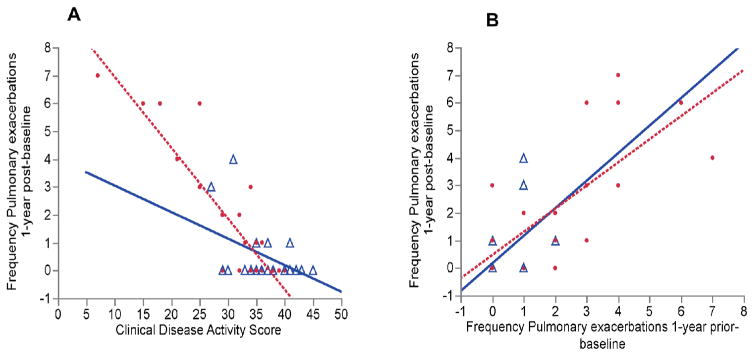
Patients in the high hs-CRP group (≥ 5.2 mg/L) demonstrated worse CDAS (r=0.67, p=0.0001) and QOL scores (r=0.57, p=0.0017) at a given FEV% predicted. In both hs-CRP groups, prior-year IV-treated PExs and baseline CDASs were significant predictors of future IV-treated PExs. Interestingly, the association between baseline CDAS and future PExs frequency was more robust in the high compared to the low hs-CRP group (r=-0.88, p<0.0001, r=-0.48, p=0.017, respectively) with a steeper regression slope (p=0.001). In addition, a significant interaction was demonstrated between elevated baseline hs-CRP levels and CDASs for the prediction of increased risk of future PExs (p=0.02). This interaction provided an additional indicator of clinical disease activity and added another dimension to the prior year PExs frequency phenotype to identify patients at increased risk for future PExs.
Stable CF patients with elevated baseline hs-CRP (≥ 5.2 mg/L) demonstrated worse clinical disease activity and QOL scores at a given level of disease severity (FEV% predicted). Elevated baseline hs-CRP values combined with clinical disease activity scores are associated with increased risk for future IV-treated PExs even in those with mild clinical disease activity scores.
在病情稳定的成年囊性纤维化(CF)患者中,我们评估了基线高敏C反应蛋白(hs-CRP)对CF临床变量以及基线后1年静脉注射(IV)治疗的肺部加重(PEx)频率的影响。
我们从成人CF中心招募了51名临床稳定的CF患者。我们将收集到的参数纳入Matouk CF临床评分和CF问卷修订后的生活质量评分(QOL)。我们将临床减去并发症的子评分用作临床疾病活动评分(CDAS)。我们根据队列中值基线hs-CRP为5.2 mg/L对患者进行二分法分类。
在给定的预测FEV%水平下,高hs-CRP组(≥5.2 mg/L)的患者表现出更差的CDAS(r = 0.67,p = 0.0001)和QOL评分(r = 0.57,p = 0.0017)。在两个hs-CRP组中,前一年IV治疗的PEx和基线CDAS都是未来IV治疗的PEx的重要预测因素。有趣的是,与低hs-CRP组相比,高hs-CRP组中基线CDAS与未来PEx频率之间的关联更强(分别为r = -0.88,p < 0.0001,r = -0.48,p = 0.017),回归斜率更陡(p = 0.001)。此外,在预测未来PEx风险增加方面,基线hs-CRP水平升高与CDAS之间存在显著交互作用(p = 0.02)。这种交互作用提供了临床疾病活动的额外指标,并为前一年PEx频率表型增加了另一个维度,以识别未来PEx风险增加的患者。
基线hs-CRP升高(≥5.2 mg/L)的稳定CF患者在给定疾病严重程度水平(预测FEV%)下表现出更差的临床疾病活动和QOL评分。即使在临床疾病活动评分较轻的患者中,基线hs-CRP值升高与临床疾病活动评分相结合也与未来IV治疗的PEx风险增加相关。