Women's Health Research Unit, Department of Obstetrics & Gynecology, Oregon Health & Science University, Portland, Oregon 97239, USA.
Curr Eye Res. 2011 Oct;36(10):867-85. doi: 10.3109/02713683.2011.594202. Epub 2011 Aug 5.
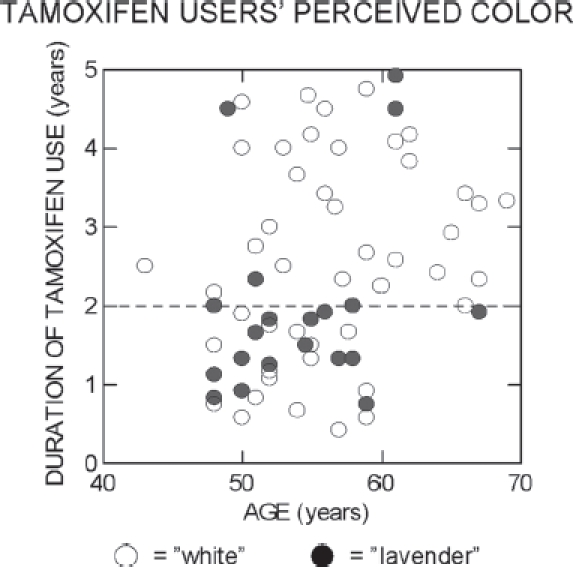
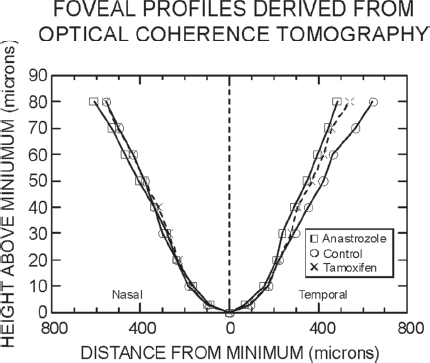
This review concerns the effects on vision and the eye of medications prescribed at three phases of treatment for women with early-stage breast cancer (BC): (1) adjuvant cytotoxic chemotherapy, (2) adjuvant endocrine therapy, and (3) symptomatic relief. The most common side effects of cytotoxic chemotherapy are epiphora and ocular surface irritation, which can be caused by any of several different regimens. Most notably, the taxane docetaxel can lead to epiphora by inducing canalicular stenosis. The selective-estrogen-receptor-modulator (SERM) tamoxifen, long the gold-standard adjuvant-endocrine-therapy for women with hormone-receptor-positive BC, increases the risk of posterior subcapsular cataract. Tamoxifen also affects the optic nerve head more often than previously thought, apparently by causing subclinical swelling within the first 2 years of use for women older than ~50 years. Tamoxifen retinopathy is rare, but it can cause foveal cystoid spaces that are revealed with spectral-domain optical coherence tomography (OCT) and that may increase the risk for macular holes. Tamoxifen often alters the perceived color of flashed lights detected via short-wavelength-sensitive (SWS) cone response isolated psychophysically; these altered perceptions may reflect a neural-response sluggishness that becomes evident at ~2 years of use. The aromatase inhibitor (AI) anastrozole affects perception similarly, but in an age-dependent manner suggesting that the change of estrogen activity towards lower levels is more important than the low estrogen activity itself. Based on analysis of OCT retinal thickness data, it is likely that anastrozole increases the tractional force between the vitreous and retina. Consequently, AI users, myopic AI users particularly, might be at increased risk for traction-related vision loss. Because bisphosphonates are sometimes prescribed to redress AI-induced bone loss, clinicians should be aware of their potential to cause scleritis and uveitis occasionally. We conclude by suggesting some avenues for future research into the visual and ocular effects of AIs, particularly as relates to assessment of cognitive function.
这篇综述主要探讨了在治疗早期乳腺癌(BC)的三个阶段中,女性患者所使用的药物对视力和眼睛的影响:(1)辅助细胞毒性化疗,(2)辅助内分泌治疗,以及(3)对症缓解。细胞毒性化疗最常见的副作用是溢泪和眼表刺激,这可能是由几种不同方案引起的。值得注意的是,紫杉烷类药物多西他赛可通过诱导泪道狭窄引起溢泪。选择性雌激素受体调节剂(SERM)他莫昔芬是激素受体阳性 BC 女性的标准辅助内分泌治疗药物,可增加后发性囊下白内障的风险。他莫昔芬还会比以前认为的更频繁地影响视神经头,这显然是由于年龄大于50 岁的女性在使用的前 2 年内出现亚临床肿胀所致。他莫昔芬性视网膜病变很少见,但它可能导致黄斑区出现中央凹囊样空间,这些病变可以通过频域光学相干断层扫描(OCT)发现,且可能增加黄斑裂孔的风险。他莫昔芬通常会改变通过短波长敏感(SWS)锥体细胞反应在心理物理上孤立检测到的闪烁光的感知颜色;这些感知变化可能反映出一种神经反应迟缓,在使用2 年后变得明显。芳香酶抑制剂(AI)阿那曲唑的影响也类似,但存在年龄依赖性,这表明雌激素活性向较低水平的变化比低雌激素活性本身更为重要。基于对 OCT 视网膜厚度数据的分析,阿那曲唑可能会增加玻璃体和视网膜之间的牵引力。因此,AI 使用者,特别是近视的 AI 使用者,可能面临与牵引相关的视力丧失的风险增加。由于双膦酸盐有时用于治疗 AI 引起的骨质流失,因此临床医生应该意识到它们偶尔会引起巩膜炎和虹膜炎的潜在风险。最后,我们建议了一些未来研究 AI 对视觉和眼部影响的途径,特别是在评估认知功能方面。