Department of Medical Intensive Care, CHU de Caen, Caen, F-14000, France.
BMC Cardiovasc Disord. 2011 Aug 8;11:48. doi: 10.1186/1471-2261-11-48.
The prediction of neurological outcome in comatose patients after cardiac arrest has major ethical and socioeconomic implications. The purpose of this study was to assess the capability of serum neuron-specific enolase (NSE), a biomarker of hypoxic brain damage, to predict death or vegetative state in comatose cardiac-arrest survivors.
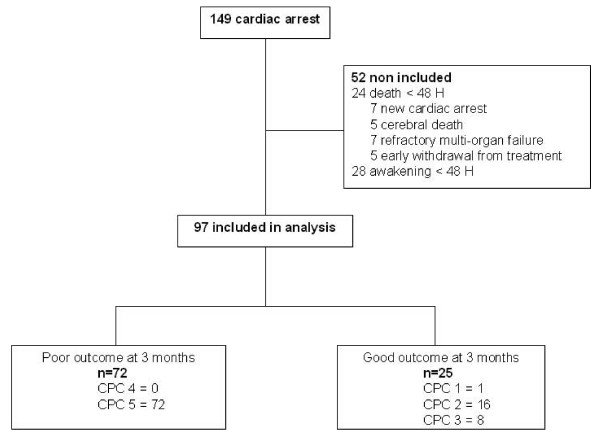
We conducted a prospective observational cohort study in one university hospital and one general hospital Intensive Care Unit (ICU). All consecutive patients who suffered cardiac arrest and were subsequently admitted from June 2007 to February 2009 were considered for inclusion in the study. Patients who died or awoke within the first 48 hours of admission were excluded from the analysis. Patients were followed for 3 months or until death after cardiopulmonary resuscitation. The Cerebral Performance Categories scale (CPC) was used as the outcome measure; a CPC of 4-5 was regarded as a poor outcome, and a CPC of 1-3 a good outcome. Measurement of serum NSE was performed at 24 h and at 72 h after the time of cardiac arrest using an enzyme immunoassay. Clinicians were blinded to NSE results.
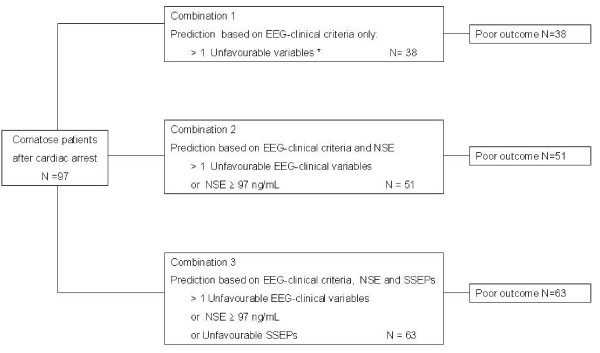
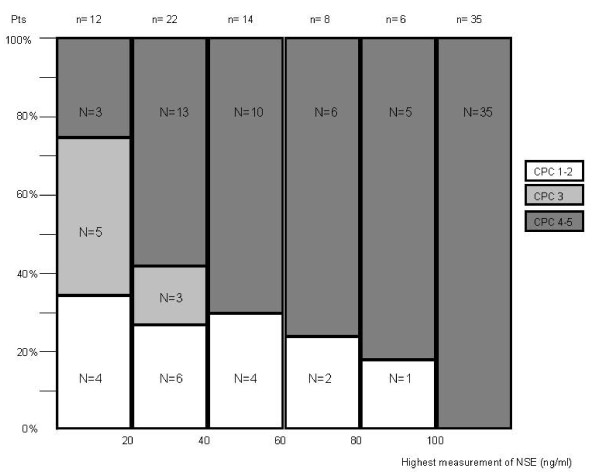
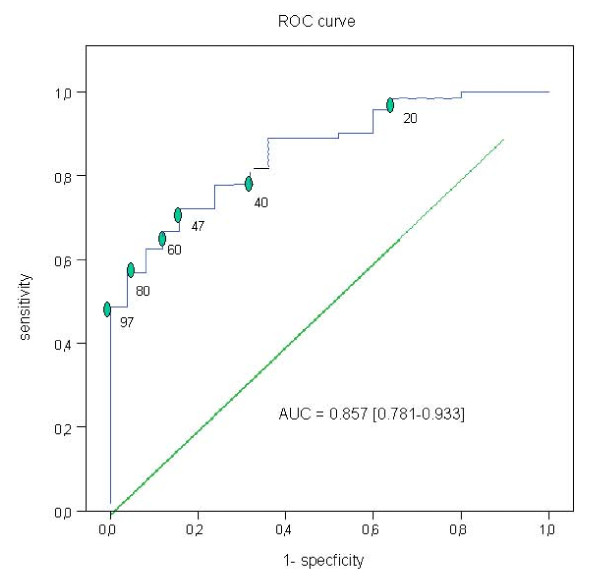
Ninety-seven patients were included. All patients were actively supported during the first days following cardiac arrest. Sixty-five patients (67%) underwent cooling after resuscitation. At 3 months 72 (74%) patients had a poor outcome (CPC 4-5) and 25 (26%) a good outcome (CPC 1-3). The median and Interquartile Range [IQR] levels of NSE at 24 h and at 72 h were significantly higher in patients with poor outcomes: NSE at 24 h: 59.4 ng/mL [37-106] versus 28.8 ng/mL [18-41] (p < 0.0001); and NSE at 72 h: 129.5 ng/mL [40-247] versus 15.7 ng/mL [12-19] (p < 0.0001). The Receiver Operator Characteristics (ROC) curve for poor outcome for the highest observed NSE value for each patient determined a cut-off value for NSE of 97 ng/mL to predict a poor neurological outcome with a specificity of 100% [95% CI = 87-100] and a sensitivity of 49% [95% CI = 37-60]. However, an approach based on a combination of SSEPs, NSE and clinical-EEG tests allowed to increase the number of patients (63/72 (88%)) identified as having a poor outcome and for whom intensive treatment could be regarded as futile.
NSE levels measured early in the course of patient care for those who remained comatose after cardiac arrest were significantly higher in patients with outcomes of death or vegetative state. In addition, we provide a cut-off value for NSE (> 97 ng/mL) with 100% positive predictive value of poor outcome. Nevertheless, for decisions concerning the continuation of treatment in this setting, we emphasize that an approach based on a combination of SSEPs, NSE and clinical EEG would be more accurate for identifying patients with a poor neurological outcome.
对于心脏骤停后昏迷的患者,神经功能预后的预测具有重大的伦理和社会经济意义。本研究旨在评估血清神经元特异性烯醇化酶(NSE)作为缺氧性脑损伤的生物标志物,预测心脏骤停后昏迷幸存者的死亡或植物状态。
我们在一家大学医院和一家综合医院的重症监护病房(ICU)进行了一项前瞻性观察队列研究。所有连续发生心脏骤停并随后于 2007 年 6 月至 2009 年 2 月入院的患者均被考虑纳入研究。入院后 48 小时内死亡或苏醒的患者被排除在分析之外。患者在心肺复苏后 3 个月或直至死亡时进行随访。使用神经功能预后量表(Cerebral Performance Categories scale,CPC)作为结局测量指标;CPC 为 4-5 表示预后不良,CPC 为 1-3 表示预后良好。在心脏骤停后 24 小时和 72 小时使用酶联免疫吸附试验测量血清 NSE 水平。临床医生对 NSE 结果进行了盲法评估。
共纳入 97 例患者。所有患者在心脏骤停后的最初几天均接受了积极的支持治疗。65 例患者(67%)在复苏后接受了降温治疗。3 个月时,72 例(74%)患者预后不良(CPC 4-5),25 例(26%)患者预后良好(CPC 1-3)。预后不良患者 24 小时和 72 小时 NSE 的中位数和四分位距(IQR)水平显著升高:24 小时 NSE:59.4ng/mL[37-106]与 28.8ng/mL[18-41](p<0.0001);72 小时 NSE:129.5ng/mL[40-247]与 15.7ng/mL[12-19](p<0.0001)。对于每位患者最高观察到的 NSE 值,ROC 曲线预测不良神经结局的截断值为 97ng/mL,特异性为 100%[95%CI=87-100],灵敏度为 49%[95%CI=37-60]。然而,基于 SSEP、NSE 和临床 EEG 测试的组合方法可以增加被识别为预后不良的患者数量(63/72(88%)),对于这些患者,强化治疗可以被认为是无效的。
心脏骤停后持续昏迷患者的 NSE 水平在死亡或植物状态结局的患者中明显升高。此外,我们提供了一个 NSE 截断值(>97ng/mL),其不良结局的阳性预测值为 100%。然而,对于在这种情况下继续治疗的决策,我们强调,基于 SSEP、NSE 和临床 EEG 的组合方法更能准确识别神经预后不良的患者。