Barbara Davis Center for Childhood Diabetes, University of Colorado Denver, Aurora, Colorado, USA.
Diabetes. 2011 Oct;60(10):2560-5. doi: 10.2337/db11-0674. Epub 2011 Aug 10.
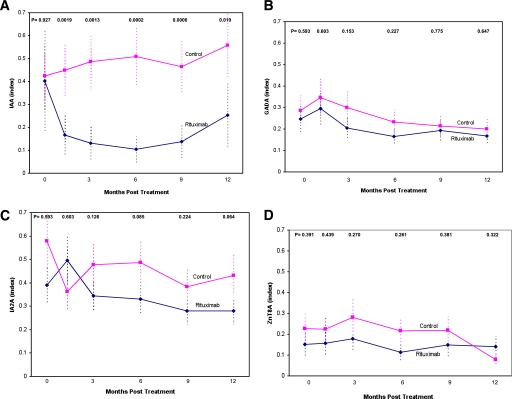
The TrialNet Study Group evaluated rituximab, a B-cell-depleting monoclonal antibody, for its effect in new-onset patients with type 1A diabetes. Rituximab decreased the loss of C-peptide over the first year of follow-up and markedly depleted B lymphocytes for 6 months after administration. This article analyzes the specific effect of rituximab on multiple islet autoantibodies.
A total of 87 patients between the ages of 8 and 40 years received either rituximab or a placebo infusion weekly for four doses close to the onset of diabetes. Autoantibodies to insulin (IAAs), GAD65 (GADAs), insulinoma-associated protein 2 (IA2As), and ZnT8 (ZnT8As) were measured with radioimmunoassays. The primary outcome for this autoantibody analysis was the mean level of autoantibodies during follow-up.
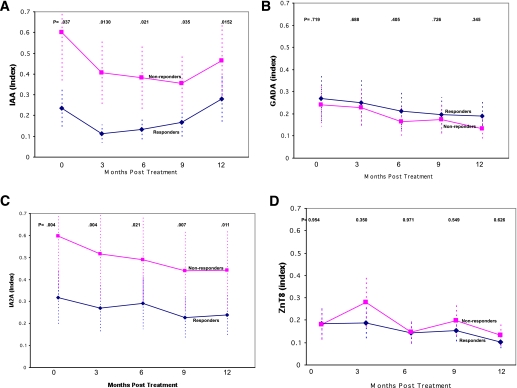
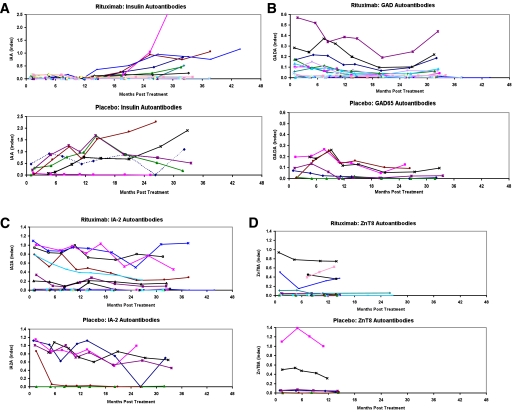
Rituximab markedly suppressed IAAs compared with the placebo injection but had a much smaller effect on GADAs, IA2As, and ZnT8As. A total of 40% (19 of 48) of rituximab-treated patients who were IAA positive became IAA negative versus 0 of 29 placebo-treated patients (P < 0.0001). In the subgroup (n = 6) treated within 50 days of diabetes, IAAs were markedly suppressed by rituximab in all patients for 1 year and for four patients as long as 3 years despite continuing insulin therapy. Independent of rituximab treatment, the mean level of IAAs at study entry was markedly lower (P = 0.035) for patients who maintained C-peptide levels during the first year of follow-up in both rituximab-treated and placebo groups.
A single course of rituximab differentially suppresses IAAs, clearly blocking IAAs for >1 year in insulin-treated patients. For the patients receiving insulin for >2 weeks prior to rituximab administration, we cannot assess whether rituximab not only blocks the acquisition of insulin antibodies induced by insulin administration and/or also suppresses preformed insulin autoantibodies. Studies in prediabetic non-insulin-treated patients will likely be needed to evaluate the specific effects of rituximab on levels of IAAs.
TrialNet 研究小组评估了利妥昔单抗(一种 B 细胞耗竭单克隆抗体)在 1 型糖尿病新发病患者中的作用。利妥昔单抗降低了随访第一年中 C 肽的损失,并在给药后 6 个月内显著耗尽 B 淋巴细胞。本文分析了利妥昔单抗对多种胰岛自身抗体的具体作用。
87 名年龄在 8 至 40 岁之间的患者在糖尿病发病后接近发病时每周接受利妥昔单抗或安慰剂输注,共 4 剂。采用放射免疫分析法测定胰岛素(IAAs)、GAD65(GADAs)、胰岛素瘤相关蛋白 2(IA2As)和锌转运蛋白 8(ZnT8As)自身抗体。该自身抗体分析的主要结果是随访期间自身抗体的平均水平。
与安慰剂注射相比,利妥昔单抗显著抑制了 IAAs,但对 GADAs、IA2As 和 ZnT8As 的影响较小。40%(19/48)的利妥昔单抗治疗的 IAA 阳性患者转为 IAA 阴性,而安慰剂治疗的 29 名患者中无 1 例(P<0.0001)。在糖尿病发病后 50 天内治疗的亚组(n=6)中,利妥昔单抗在所有患者中在 1 年内明显抑制了 IAAs,4 例患者在 3 年内也明显抑制了 IAAs,尽管继续胰岛素治疗。无论利妥昔单抗治疗与否,在利妥昔单抗治疗组和安慰剂组中,在随访的第一年中持续保持 C 肽水平的患者的 IAAs 平均水平在研究入组时明显更低(P=0.035)。
单次利妥昔单抗治疗可显著抑制 IAAs,在接受胰岛素治疗的患者中明显阻断 IAAs 超过 1 年。对于在利妥昔单抗给药前接受胰岛素治疗超过 2 周的患者,我们无法评估利妥昔单抗是否不仅阻断了胰岛素给药诱导的胰岛素抗体的获得,而且还抑制了预先形成的胰岛素自身抗体。可能需要在非胰岛素治疗的糖尿病前期患者中进行研究,以评估利妥昔单抗对 IAAs 水平的具体影响。