Department of Medical Psychology & Sociology, University of Göttingen, Waldweg 37, 37073 Göttingen, Germany.
BMC Med Res Methodol. 2011 Aug 12;11:114. doi: 10.1186/1471-2288-11-114.
Based on the general approach of locus of control, health locus of control (HLOC) concerns control-beliefs due to illness, sickness and health. HLOC research results provide an improved understanding of health related behaviour and patients' compliance in medical care. HLOC research distinguishes between beliefs due to Internality, Externality powerful Others (POs) and Externality Chance. However, evidences for differentiating the POs dimension were found. Previous factor analyses used selected and predominantly clinical samples, while non-clinical studies are rare. The present study is the first analysis of the HLOC structure based on a large representative general population sample providing important information for non-clinical research and public health care.
The standardised German questionnaire which assesses HLOC was used in a representative adult general population sample for a region in Northern Germany (N = 4,075). Data analyses used ordinal factor analyses in LISREL and Mplus. Alternative theory-driven models with one to four latent variables were compared using confirmatory factor analysis. Fit indices, chi-square difference tests, residuals and factor loadings were considered for model comparison. Exploratory factor analysis was used for further model development. Results were cross-validated splitting the total sample randomly and using the cross-validation index.
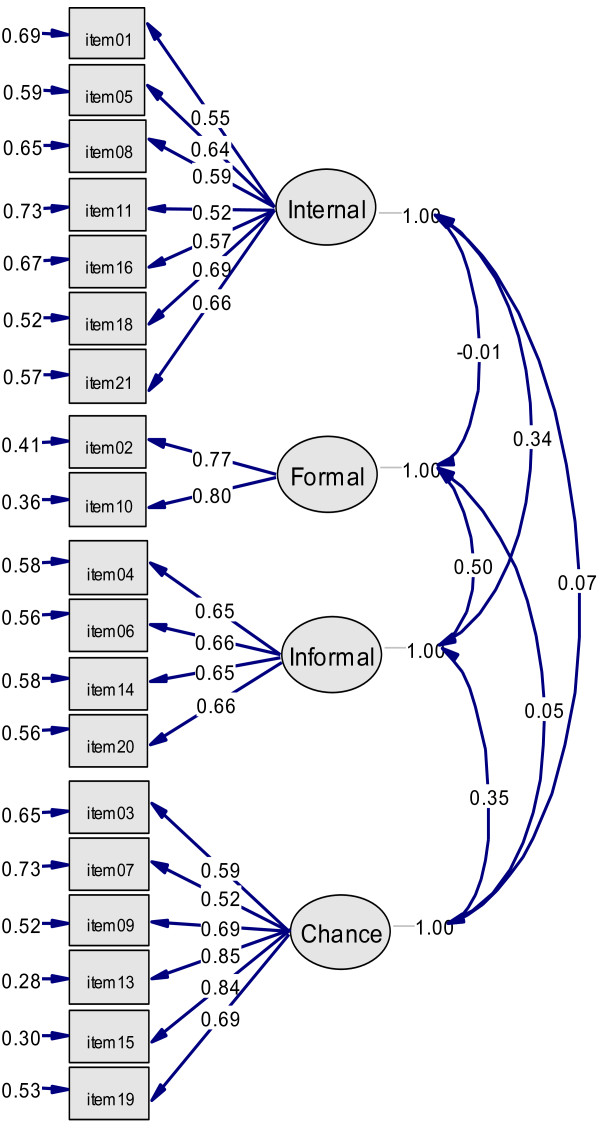
A model with four latent variables (Internality, Formal Help, Informal Help and Chance) best represented the HLOC construct (three-dimensional model: normed chi-square = 9.55; RMSEA = 0.066; CFI = 0.931; SRMR = 0.075; four-dimensional model: normed chi-square = 8.65; RMSEA = 0.062; CFI = 0.940; SRMR = 0.071; chi-square difference test: p < 0.001). After excluding one item, the superiority of the four- over the three-dimensional HLOC construct became very obvious (three-dimensional model: normed chi-square = 7.74; RMSEA = 0.059; CFI = 0.950; SRMR = 0.079; four-dimensional model: normed chi-square = 5.75; RMSEA = 0.049; CFI = 0.965; SRMR = 0.065; chi-square difference test: p < 0.001). Results were confirmed by cross-validation. Results based on our large community sample indicated that western general populations separate health-related control-beliefs concerning formal and informal assistance.
Future non-clinical HLOC studies in western cultures should consider four dimensions of HLOC: Internality, Formal Help, Informal Help and Chance. However, the standardised German instrument needs modification. Therefore, confirmation of our results may be useful. Future research should compare HLOC structure between clinical and non-clinical samples as well as cross-culturally.
基于控制源的一般方法,健康控制源(HLOC)关注与疾病、疾病和健康相关的控制信念。HLOC 研究结果提供了对与健康相关的行为和患者在医疗保健中的依从性的更好理解。HLOC 研究区分了内在性、外在性(强大的他人(POs)和偶然性)的信念。然而,已经发现了区分 POs 维度的证据。以前的因素分析使用了选定的和主要是临床样本,而很少有非临床研究。本研究是基于德国北部一个代表性的成人一般人群样本对 HLOC 结构的首次分析,为非临床研究和公共卫生保健提供了重要信息。
使用评估 HLOC 的标准化德语问卷对德国北部一个地区的代表性成年一般人群样本(N=4075)进行了调查。数据分析使用 LISREL 和 Mplus 中的有序因子分析。使用验证性因子分析比较了具有一个到四个潜在变量的替代理论驱动模型。模型比较考虑了拟合指数、卡方差异检验、残差和因子负荷。探索性因子分析用于进一步的模型开发。通过随机分割总样本并使用交叉验证指数,对结果进行了交叉验证。
一个具有四个潜在变量(内在性、正式帮助、非正式帮助和偶然性)的模型最好地代表了 HLOC 结构(三维模型:规范卡方=9.55;RMSEA=0.066;CFI=0.931;SRMR=0.075;四维模型:规范卡方=8.65;RMSEA=0.062;CFI=0.940;SRMR=0.071;卡方差异检验:p<0.001)。排除一个项目后,四维度 HLOC 结构的优越性变得非常明显(三维模型:规范卡方=7.74;RMSEA=0.059;CFI=0.950;SRMR=0.079;四维模型:规范卡方=5.75;RMSEA=0.049;CFI=0.965;SRMR=0.065;卡方差异检验:p<0.001)。交叉验证结果得到了确认。基于我们大型社区样本的结果表明,西方普通人群将与正式和非正式帮助相关的健康相关控制信念分开。
未来西方文化中的非临床 HLOC 研究应考虑 HLOC 的四个维度:内在性、正式帮助、非正式帮助和偶然性。然而,标准化的德语工具需要修改。因此,我们的结果可能是有用的。未来的研究应该比较临床和非临床样本以及跨文化之间的 HLOC 结构。