US Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Bureau, 5600 Fishers Lane, Room 18-41, Rockville, MD 20857, USA.
J Community Health. 2012 Apr;37(2):412-20. doi: 10.1007/s10900-011-9458-3.
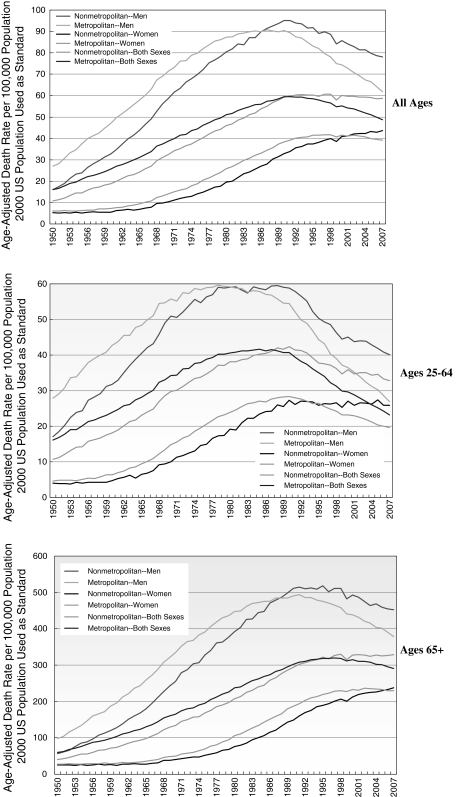
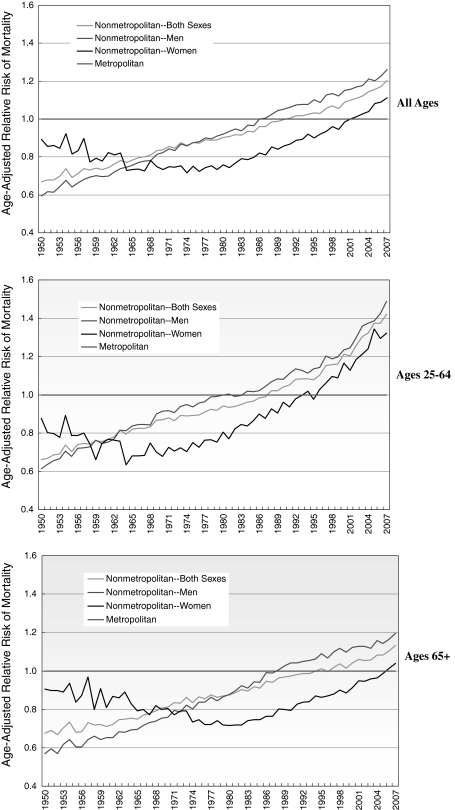
This study examined disparities in lung cancer mortality rates among US men and women in metropolitan and non-metropolitan areas from 1950 through 2007. Annual age-adjusted mortality rates were calculated for men and women in metropolitan and non-metropolitan areas, and differences in mortality rates were tested for statistical significance. Log-linear regression was used to model annual rates of change in mortality over time, while Poisson regression was used to estimate relative risk after adjusting for age, sex, deprivation, and urbanization levels. Urbanization patterns in lung cancer mortality changed dramatically between 1950 and 2007. Compared to men in metropolitan areas, men aged 25-64 years in non-metropolitan areas had significantly lower lung cancer mortality rates from 1950 to 1977 and men aged ≥65 years in non-metropolitan areas had lower mortality rates from 1950 to 1985. Differentials began to reverse and widen by the mid-1980s for men and by the mid-1990s for younger women. In 2007, compared to their metropolitan counterparts, men aged 25-64 and ≥65 years in non-metropolitan areas had 49 and 19% higher lung cancer mortality and women aged 25-64 and ≥65 years in non-metropolitan areas had 32 and 4% higher lung cancer mortality, respectively. Although adjustment for deprivation levels reduced excess lung cancer mortality risk among those in non-metropolitan areas, significant rural-urban differences remained. Rural-urban patterns reversed because of faster and earlier reductions in lung cancer mortality among men and women in metropolitan areas. Temporal trends in rural-urban disparities in lung cancer mortality appear to be consistent with those in smoking.
这项研究调查了 1950 年至 2007 年美国城乡地区男性和女性肺癌死亡率的差异。为城乡地区的男性和女性计算了年度年龄调整死亡率,并对死亡率差异进行了统计学意义检验。对数线性回归用于对死亡率随时间的年度变化率进行建模,而泊松回归用于在调整年龄、性别、贫困和城市化水平后估计相对风险。1950 年至 2007 年,肺癌死亡率的城市化模式发生了巨大变化。与城市地区的男性相比,1950 年至 1977 年,25-64 岁的非城市地区男性肺癌死亡率明显较低,1950 年至 1985 年,65 岁以上的非城市地区男性死亡率较低。从 20 世纪 80 年代中期开始,男性的差异开始逆转和扩大,而年轻女性则在 90 年代中期开始逆转和扩大。2007 年,与城市地区的同龄人相比,25-64 岁和≥65 岁的非城市地区男性的肺癌死亡率分别高出 49%和 19%,25-64 岁和≥65 岁的非城市地区女性的肺癌死亡率分别高出 32%和 4%。尽管调整贫困水平降低了非城市地区人群的肺癌超额死亡率风险,但城乡差异仍然显著。城乡差异模式发生逆转,是因为城市地区男性和女性的肺癌死亡率下降更快、更早。城乡肺癌死亡率差异的时间趋势似乎与吸烟趋势一致。