Division of Population, Health Sciences and Education, St George's University of London, UK.
BMJ. 2011 Aug 25;343:d4920. doi: 10.1136/bmj.d4920.
To develop a novel prognostic indicator for use in patients with advanced cancer that is significantly better than clinicians' estimates of survival.
Prospective multicentre observational cohort study.
18 palliative care services in the UK (including hospices, hospital support teams, and community teams).
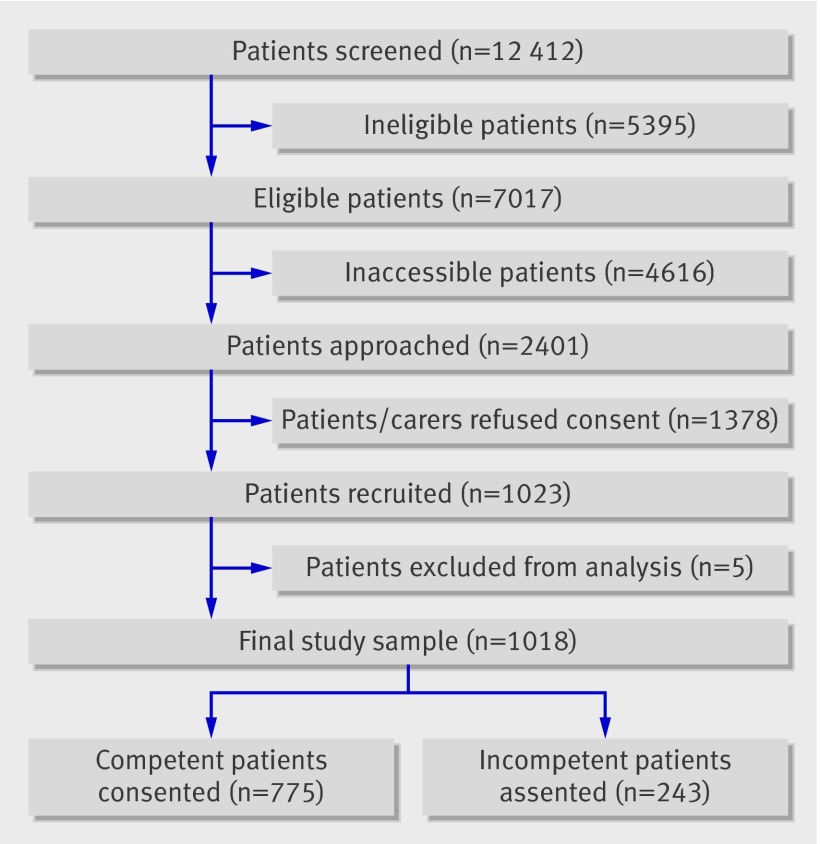
1018 patients with locally advanced or metastatic cancer, no longer being treated for cancer, and recently referred to palliative care services.
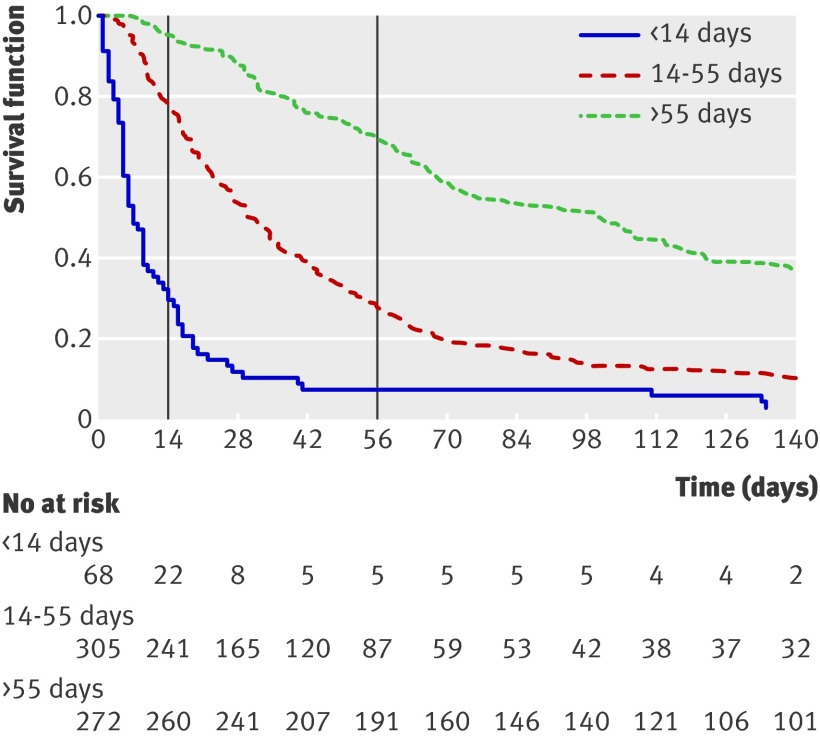
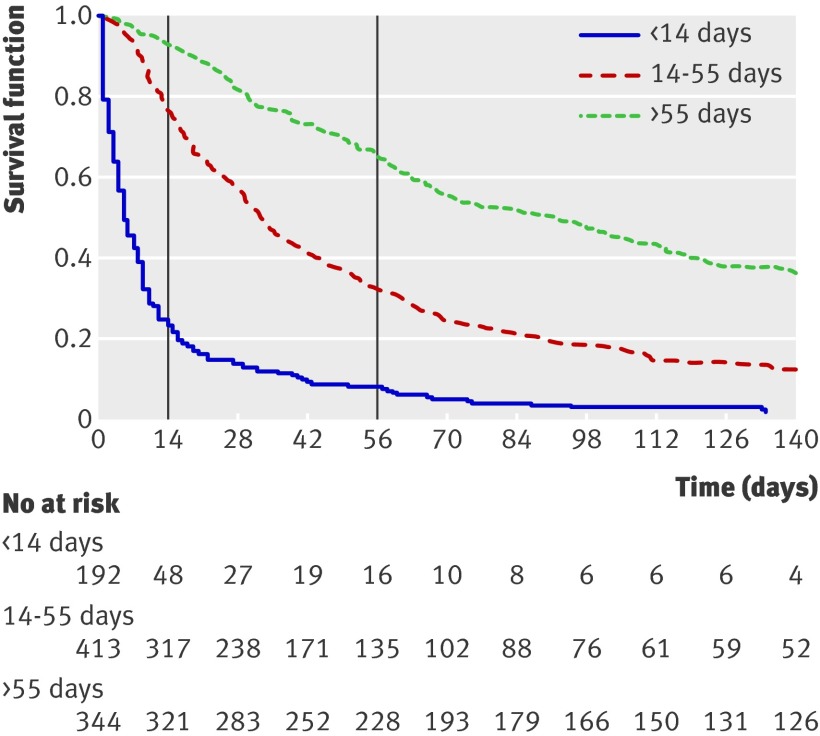
Performance of a composite model to predict whether patients were likely to survive for "days" (0-13 days), "weeks" (14-55 days), or "months+" (>55 days), compared with actual survival and clinicians' predictions.
On multivariate analysis, 11 core variables (pulse rate, general health status, mental test score, performance status, presence of anorexia, presence of any site of metastatic disease, presence of liver metastases, C reactive protein, white blood count, platelet count, and urea) independently predicted both two week and two month survival. Four variables had prognostic significance only for two week survival (dyspnoea, dysphagia, bone metastases, and alanine transaminase), and eight variables had prognostic significance only for two month survival (primary breast cancer, male genital cancer, tiredness, loss of weight, lymphocyte count, neutrophil count, alkaline phosphatase, and albumin). Separate prognostic models were created for patients without (PiPS-A) or with (PiPS-B) blood results. The area under the curve for all models varied between 0.79 and 0.86. Absolute agreement between actual survival and PiPS predictions was 57.3% (after correction for over-optimism). The median survival across the PiPS-A categories was 5, 33, and 92 days and survival across PiPS-B categories was 7, 32, and 100.5 days. All models performed as well as, or better than, clinicians' estimates of survival.
In patients with advanced cancer no longer being treated, a combination of clinical and laboratory variables can reliably predict two week and two month survival.
开发一种新的预后指标,用于预测晚期癌症患者的生存情况,其预测效果显著优于临床医生的估计。
前瞻性多中心观察队列研究。
英国 18 个姑息治疗服务机构(包括临终关怀医院、医院支持团队和社区团队)。
1018 名局部晚期或转移性癌症患者,这些患者已不再接受癌症治疗,且刚被转至姑息治疗服务机构。
与实际生存情况和临床医生的预测相比,预测患者是否有可能在“天”(0-13 天)、“周”(14-55 天)或“月+”(>55 天)内存活的复合模型的性能。
多变量分析显示,11 项核心变量(脉搏率、总体健康状况、智力测试评分、体能状态、厌食症、转移性疾病的任何部位、肝转移、C 反应蛋白、白细胞计数、血小板计数和尿素)可独立预测两周和两个月的生存情况。四项变量仅对两周的生存情况具有预后意义(呼吸困难、吞咽困难、骨转移和丙氨酸氨基转移酶),八项变量仅对两个月的生存情况具有预后意义(原发性乳腺癌、男性生殖系统癌症、乏力、体重减轻、淋巴细胞计数、中性粒细胞计数、碱性磷酸酶和白蛋白)。为无(PiPS-A)和有(PiPS-B)血液检查结果的患者分别建立了单独的预后模型。所有模型的曲线下面积在 0.79 至 0.86 之间。实际生存情况与 PiPS 预测值之间的绝对一致性为 57.3%(经校正后,存在过度乐观的情况)。PiPS-A 各分类的中位生存时间为 5、33 和 92 天,PiPS-B 各分类的中位生存时间为 7、32 和 100.5 天。所有模型的表现均与临床医生的生存估计相当,甚至优于临床医生的估计。
对于不再接受治疗的晚期癌症患者,临床和实验室变量的组合可以可靠地预测两周和两个月的生存情况。