Department of Medicine, University of California, San Francisco, USA.
AIDS. 2011 Nov 13;25(17):2123-31. doi: 10.1097/QAD.0b013e32834c4ac1.
To assess whether T-cell activation independently predicts the extent of CD4(+) T-cell recovery and mortality in HIV-infected Ugandans initiating antiretroviral therapy (ART).
Prospective cohort study.
HIV-infected adults starting ART and achieving a plasma HIV RNA level (VL) less than 400 copies/ml by month 6 were sampled from the Uganda AIDS Rural Treatment Outcomes (UARTO) cohort in Mbarara, Uganda. CD4 count, VL, and the percentage-activated (CD38(+)HLA-DR(+)) T cells were measured every 3 months.
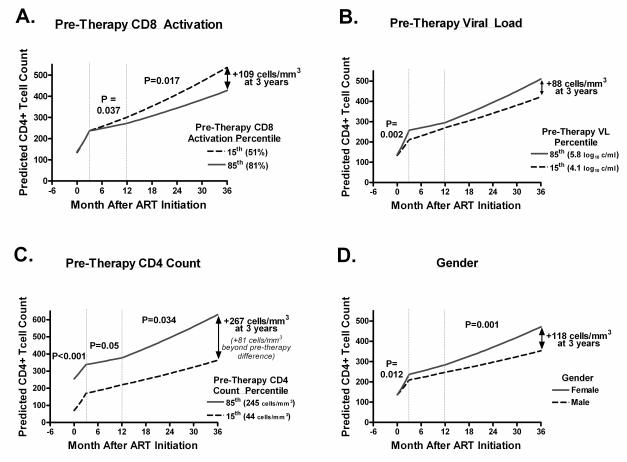
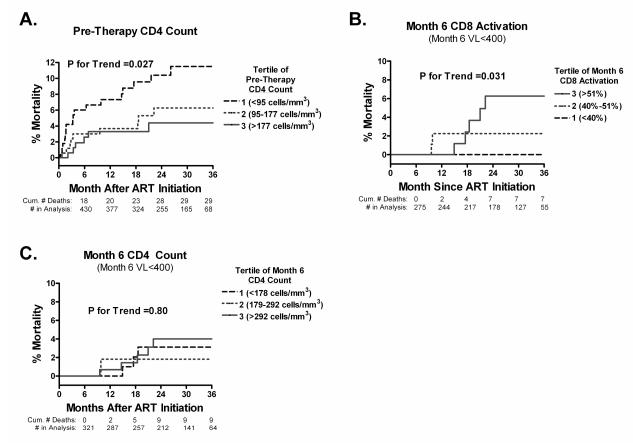
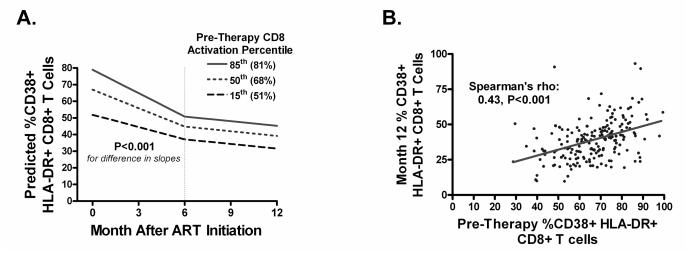
Of 451 HIV-infected Ugandans starting ART, most were women (70%) with median pre-ART values: age, 34 years; CD4 count, 135 cells/μl; and VL, 5.1 log(10) copies/ml. Of these, 93% achieved a VL less than 400 copies/ml by month 6 and were followed for a median of 24 months, with 8% lost to follow-up at 3 years. Higher pre-ART CD8(+) T-cell activation was associated with diminished CD4 recovery after year 1, after adjustment for pre-ART CD4 count, VL, and sex (P = 0.017). Thirty-four participants died, 15 after month 6. Each 10% point increase in activated CD8(+) T cells at month 6 of suppressive ART was associated with a 1.6-fold increased hazard of subsequent death after adjusting for pretherapy CD4 count (P = 0.048).
Higher pre-ART CD8(+) T-cell activation independently predicts slower CD4(+) T-cell recovery and higher persistent CD8(+) T-cell activation during ART-mediated viral suppression independently predicts increased mortality among HIV-infected Ugandans. Novel therapeutic strategies aimed at preventing or reversing immune activation during ART are needed in this setting.
评估 T 细胞激活是否能独立预测开始抗逆转录病毒治疗(ART)的 HIV 感染者 CD4(+)T 细胞恢复程度和死亡率。
前瞻性队列研究。
从乌干达 Mbarara 的乌干达艾滋病农村治疗结果(UARTO)队列中抽取开始接受 ART 且在第 6 个月时血浆 HIV RNA 水平(VL)低于 400 拷贝/ml 的 HIV 感染者成年人作为研究对象。每 3 个月检测一次 CD4 计数、VL 和激活的 T 细胞百分比(CD38(+)HLA-DR(+))。
在 451 名开始接受 ART 的 HIV 感染者中,大多数为女性(70%),中位基线值为:年龄 34 岁,CD4 计数 135 个/μl,VL 为 5.1log10 拷贝/ml。其中,93%的患者在第 6 个月时 VL 低于 400 拷贝/ml,并随访中位时间 24 个月,3 年后有 8%的患者失访。调整基线 CD4 计数、VL 和性别后,较高的基线 CD8(+)T 细胞激活与第 1 年以后的 CD4 恢复减少相关(P = 0.017)。有 34 名患者死亡,其中 15 名在第 6 个月后死亡。在调整基线 CD4 计数后,在 ART 抑制病毒的第 6 个月时,激活的 CD8(+)T 细胞每增加 10%,随后死亡的风险增加 1.6 倍(P = 0.048)。
较高的基线 CD8(+)T 细胞激活独立预测 CD4(+)T 细胞恢复较慢,ART 期间持续较高的 CD8(+)T 细胞激活独立预测 HIV 感染者死亡率增加。在这种情况下,需要有新的治疗策略来预防或逆转 ART 期间的免疫激活。