Department of Psychiatry, Dartmouth Medical School, VA Medical Center, 215 North Main Street, White River Junction, VT 05009, USA.
BMC Psychiatry. 2011 Sep 9;11:146. doi: 10.1186/1471-244X-11-146.
The development of hospital service areas (HSAs) using small area analysis has been useful in examining variation in medical and surgical care; however, the techniques of small area analysis are underdeveloped in understanding psychiatric admission rates. We sought to develop these techniques in order to understand the relationship between psychiatric bed supply and admission rates in Northern New England. Our primary hypotheses were that there would be substantial variation in psychiatric admission across geographic settings and that bed availability would be positively correlated with admission rates, reflecting a supplier-induced demand phenomenon. Our secondary hypothesis was that the construction of psychiatric HSAs (PHSAs) would yield more meaningful results than the use of existing general medical hospital service areas.
To address our hypotheses, we followed a four-step analytic process: 1) we used small area analytic techniques to define our PHSAs, 2) we calculated the localization index for PHSAs and compared that to the localization index for general medical HSAs, 3) we used the number of psychiatric hospital beds, the number of psychiatric admissions, and census data to calculate population-based bed-supply and psychiatric admission rates for each PHSA, and 4) we correlated population-based admission rates to population-based psychiatric bed supply.
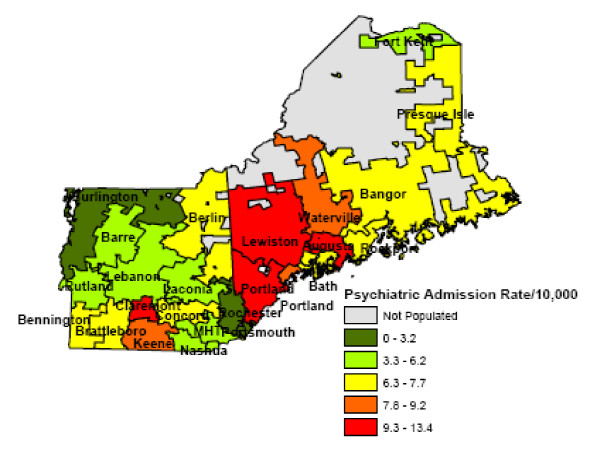
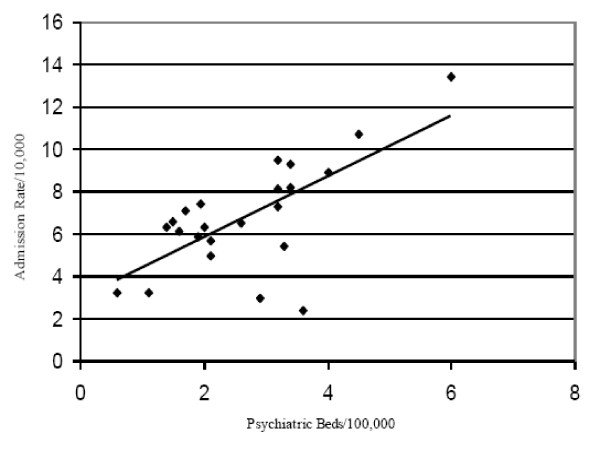
The admission rate for psychiatric diagnosis varied considerably among the PHSAs, with rates varying from 2.4 per 100,000 in Portsmouth, NH to 13.4 per 100,000 in Augusta, ME. There was a positive correlation of 0.71 between a PHSA's supply of beds and admission rate. Using our PSHAs produced a substantially higher localization index than using general medical hospital services areas (0.69 vs. 0.23), meaning that our model correctly predicted geographic utilization at three times the rate of the existing model.
The positive correlation between admission and bed supply suggests that psychiatric bed availability may partially explain the variation in admission rates. Development of PHSAs, rather than relying on the use of established general medical HSAs, improves the relevance and accuracy of small area analysis in understanding mental health services utilization.
使用小区域分析方法来开发医院服务区(HSAs)有助于检查医疗和手术护理的变化;然而,小区域分析技术在理解精神科入院率方面还不够发达。我们试图开发这些技术,以便了解新英格兰北部地区的精神科床位供应与入院率之间的关系。我们的主要假设是,在地理环境方面,精神科入院率会有很大的差异,床位的可利用性与入院率呈正相关,反映了供应商诱导的需求现象。我们的次要假设是,构建精神科 HSA(PHSA)将比使用现有的一般医疗医院服务区产生更有意义的结果。
为了验证我们的假设,我们遵循了一个四步分析过程:1)我们使用小区域分析技术来定义我们的 PHSAs;2)我们计算了 PHSAs 的本地化指数,并将其与一般医疗 HSA 的本地化指数进行了比较;3)我们使用精神科医院床位数量、精神科入院人数和人口普查数据,计算了每个 PHSA 的基于人口的床位供应和精神科入院率;4)我们将基于人口的入院率与基于人口的精神科床位供应相关联。
PHSA 之间的精神科诊断入院率差异很大,从新罕布什尔州朴茨茅斯的每 10 万人 2.4 例到缅因州奥古斯塔的每 10 万人 13.4 例。PHSA 的床位供应与入院率之间存在 0.71 的正相关关系。使用我们的 PSHAs 产生的本地化指数明显高于使用一般医疗医院服务区域(0.69 对 0.23),这意味着我们的模型正确预测了现有模型的三倍的地理利用。
入院率与床位供应之间的正相关表明,精神科床位的可获得性可能部分解释了入院率的变化。开发 PHSAs,而不是依赖于使用现有的一般医疗 HSA,可以提高小区域分析在理解精神卫生服务利用方面的相关性和准确性。