Department of Histopathology, Bristol Royal Infirmary, Bristol BS2 8HW, UK.
BMC Cancer. 2011 Sep 12;11:390. doi: 10.1186/1471-2407-11-390.
Overexpression of carbonic anhydrase (CA IX) is associated with poor survival in several adult-type cancers but its expression is undocumented in Wilms tumour (WT), the most common tumour of the paediatric kidney.
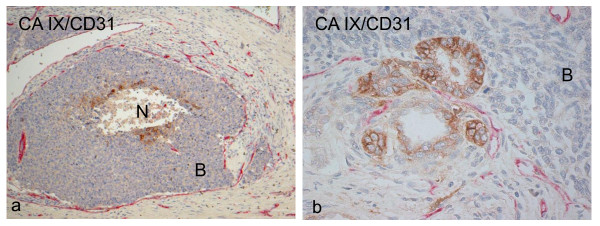
CA9 expression was measured using polymerase chain reaction (PCR) in 13 WTs and matched-paired non-neoplastic kidneys (NKs). CA IX and hypoxia-inducible factor-1 α-subunit (HIF-1α) protein were quantified in 15 matched-paired WTs and NKs using enzyme-linked immunosorbent assays. CA IX and HIF-1α were localised by immunostaining tissue sections of 70 WTs (untreated WTs, n = 22; chemotherapy-treated WTs, n = 40; relapsed/metastatic WTs, n = 8). CA IX-positive untreated WTs (n = 14) were immunostained for vascular endothelial growth factor (VEGF), glucose transporter-1 (GLUT1) and CD31. Double staining for CA IX and CD31 was performed in WTs (n = 14).
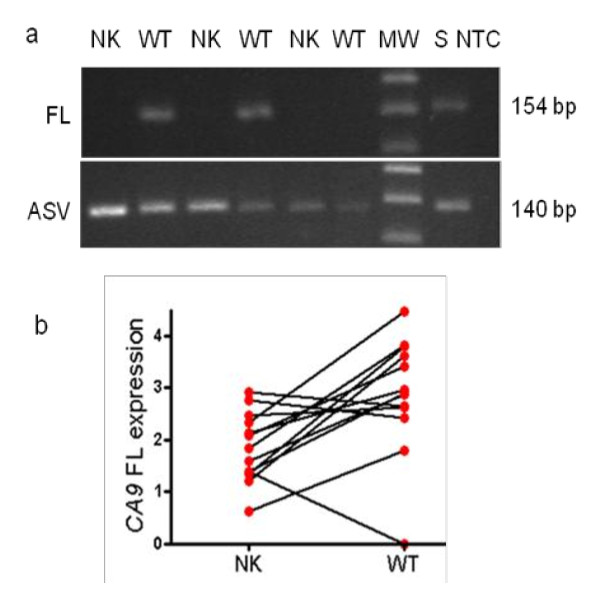
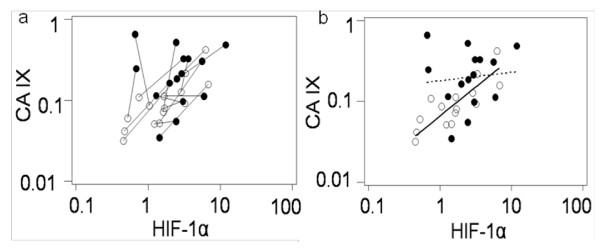
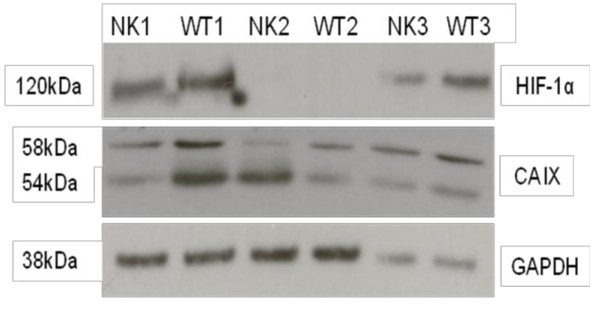
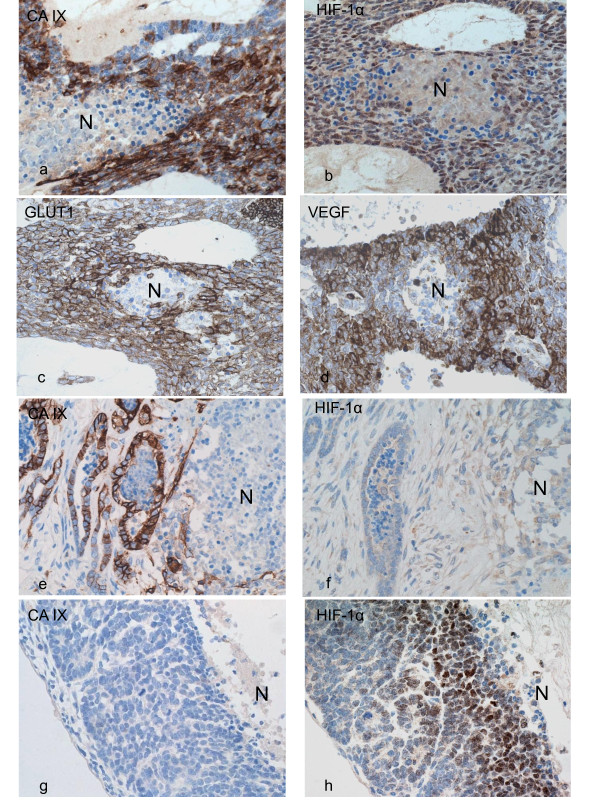
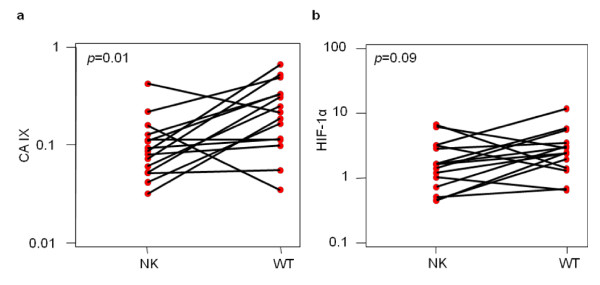
CA9 full length (FL) was significantly up-regulated in WTs compared to NKs (p = 0.009) by real-time PCR. Conventional PCR showed expression of alternative splice variant in all NKs and WTs but FL in WTs only. WTs showed a 2-fold increase in CA IX protein over NKs (p = 0.01). HIF-1α levels were up-regulated in WTs compared to NKs, although the difference was not statistically significant (p = 0.09). CA IX and HIF-1α immunolocalisation were observed in 63% and 93% of WTs, respectively. The median fraction of cells staining positively for CA IX and HIF-1α was 5% and 22%, respectively. There was no significant association between the expression of either CA IX or HIF-1α and clinicopathological variables in WTs resected following chemotherapy. VEGF and GLUT1 immunoreactivity was seen in 94% and 100% with the median fraction of 10% and 60% respectively. Co-expression and co-localisation of all four hypoxia markers was seen in 7/14 and 6/14 cases respectively. CA IX was seen in well vascularised areas as well as in the peri-necrotic areas.
Carbonic anhydrase 9 (mRNA and protein), and HIF-1α protein are overexpressed in a significant portion of WTs. No significant association was detected between the expression of either CA IX or HIF-1α and clinicopathological variables in WTs resected following chemotherapy. Cellular localisation studies in untreated WTs suggest that CA IX and HIF-1α are regulated by hypoxia and non-hypoxia mechanisms.
碳酸酐酶(CA)IX 的过表达与几种成人型癌症的不良预后相关,但在小儿肾脏最常见的肿瘤——Wilms 瘤(WT)中,其表达尚未被记录。
采用聚合酶链反应(PCR)检测 13 例 WT 和配对非肿瘤性肾脏(NK)中的 CA9 表达。采用酶联免疫吸附试验(ELISA)检测 15 例配对 WT 和 NK 中的 CA IX 和缺氧诱导因子-1α亚单位(HIF-1α)蛋白。采用免疫组化检测 70 例 WT(未治疗 WT,n=22;化疗治疗 WT,n=40;复发/转移 WT,n=8)的组织切片中 CA IX 和 HIF-1α的定位。对 14 例 CA IX 阳性未治疗 WT 进行血管内皮生长因子(VEGF)、葡萄糖转运蛋白-1(GLUT1)和 CD31 的免疫染色。对 14 例 WT 进行 CA IX 和 CD31 的双重染色。
实时 PCR 显示,WT 中 CA9 全长(FL)明显高于 NK(p=0.009)。常规 PCR 显示所有 NK 和 WT 均存在选择性剪接变体表达,但 WT 仅存在 FL。WT 中 CA IX 蛋白的表达比 NK 高 2 倍(p=0.01)。与 NK 相比,WT 中 HIF-1α 水平升高,但差异无统计学意义(p=0.09)。CA IX 和 HIF-1α 的免疫定位分别在 63%和 93%的 WT 中观察到。CA IX 和 HIF-1α 阳性细胞的中位数比例分别为 5%和 22%。WT 切除化疗后,CA IX 或 HIF-1α 的表达与临床病理变量之间无显著相关性。VEGF 和 GLUT1 免疫反应分别在 94%和 100%的病例中观察到,中位数比例分别为 10%和 60%。4 种缺氧标志物的共表达和共定位分别在 7/14 和 6/14 例中观察到。CA IX 见于血管丰富区和坏死区周围。
碳酸酐酶 9(mRNA 和蛋白)和 HIF-1α 蛋白在 WT 的大部分中过度表达。WT 切除化疗后,CA IX 或 HIF-1α 的表达与临床病理变量之间无显著相关性。未治疗 WT 的细胞定位研究表明,CA IX 和 HIF-1α 受缺氧和非缺氧机制的调节。