Ann Arbor, Mich.; Pittsburgh and Shohola, Pa.; St. Paul, Minn.; Dallas, Texas; Arlington Heights, Ill.; and New York, N.Y. From the Section of Plastic Surgery, University of Michigan; Division of Plastic and Reconstructive Surgery, University of Pittsburgh; Department of Plastic and Hand Surgery, Regions Hospital; Department of Plastic Surgery, University of Texas Southwestern; JBH Consulting; American Society of Plastic Surgeons; and Plastic and Reconstructive Surgery Service, Memorial Sloan-Kettering Cancer Center.
Plast Reconstr Surg. 2012 Jan;129(1):160-168. doi: 10.1097/PRS.0b013e318236215c.
The risk of postoperative bleeding is the chief concern expressed by plastic surgeons who do not use pharmacologic prophylaxis against venous thromboembolism. The Plastic Surgery Foundation-funded Venous Thromboembolism Prevention Study examined whether receipt of postoperative enoxaparin prophylaxis changed 60-day reoperative hematoma rates.
In 2009, the study's network sites uniformly adopted a "best practice" clinical protocol to provide postoperative enoxaparin to adult plastic surgery patients at risk for perioperative venous thromboembolism. Historical control patients (2006 to 2008) received no chemoprophylaxis for 60 days after surgery. Retrospective chart review identified demographic and surgery-specific risk factors that potentially contributed to bleeding risk. The primary study outcome was 60-day reoperative hematoma. Stratified analyses examined reoperative hematoma in the overall population and among high-risk patients. Multivariable logistic regression controlled for identified confounders.
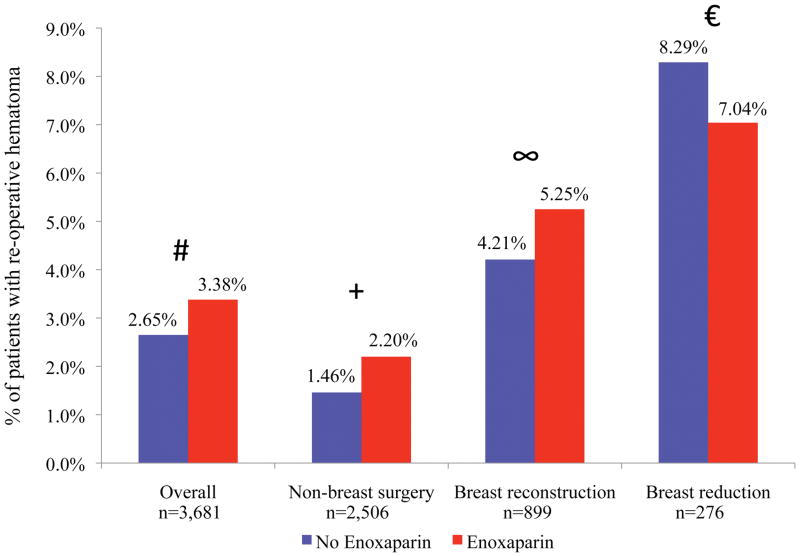
Complete data were available for 3681 patients (2114 controls and 1567 enoxaparin patients). Overall, postoperative enoxaparin did not change the reoperative hematoma rate when compared with controls (3.38 percent versus 2.65 percent, p = 0.169). Similar results were seen in subgroup analyses for breast reconstruction (5.25 percent versus 4.21 percent, p = 0.737), breast reduction (7.04 percent versus 8.29 percent, p = 0.194), and nonbreast plastic surgery (2.20 percent versus 1.46 percent, p = 0.465). In the regression model, independent predictors of reoperative hematoma included breast surgery, microsurgical procedure, and post-bariatric surgery body contouring. Receipt of postoperative enoxaparin was not an independent predictor (odds ratio, 1.16; 95 percent CI, 0.77 to 1.76).
Postoperative enoxaparin does not produce a clinically relevant or statistically significant increase in observed rates of reoperative hematoma.
CLINICAL QUESTION/LEVEL OF EVIDENCE: Risk: II.
对于不使用药物预防静脉血栓栓塞症的整形医生来说,术后出血的风险是他们最关心的问题。由整形外科学基金会资助的静脉血栓栓塞症预防研究调查了接受术后依诺肝素预防是否会改变 60 天再次手术血肿的发生率。
2009 年,该研究的网络站点统一采用“最佳实践”临床方案,为有围手术期静脉血栓栓塞风险的成人整形手术患者提供术后依诺肝素。回顾性图表审查确定了可能导致出血风险的人口统计学和手术特异性危险因素。主要研究结果是 60 天的再次手术血肿。分层分析检查了总体人群和高危人群中的再次手术血肿。多变量逻辑回归控制了已确定的混杂因素。
共有 3681 例患者(2114 例对照组和 1567 例依诺肝素组)的数据完整。总体而言,与对照组相比,术后依诺肝素并未改变再次手术血肿的发生率(3.38%比 2.65%,p=0.169)。在乳房重建(5.25%比 4.21%,p=0.737)、乳房缩小(7.04%比 8.29%,p=0.194)和非乳房整形手术(2.20%比 1.46%,p=0.465)的亚组分析中也得到了类似的结果。在回归模型中,再次手术血肿的独立预测因素包括乳房手术、显微手术和减肥手术后的身体轮廓。接受术后依诺肝素不是独立的预测因素(比值比,1.16;95%置信区间,0.77 至 1.76)。
术后依诺肝素不会导致观察到的再次手术血肿发生率出现临床相关或统计学显著增加。
临床问题/证据水平:风险:II 级。