GF Strong Rehabilitation Centre, Vancouver, BC, Canada.
Dysphagia. 2012 Sep;27(3):297-306. doi: 10.1007/s00455-011-9366-9. Epub 2011 Sep 18.
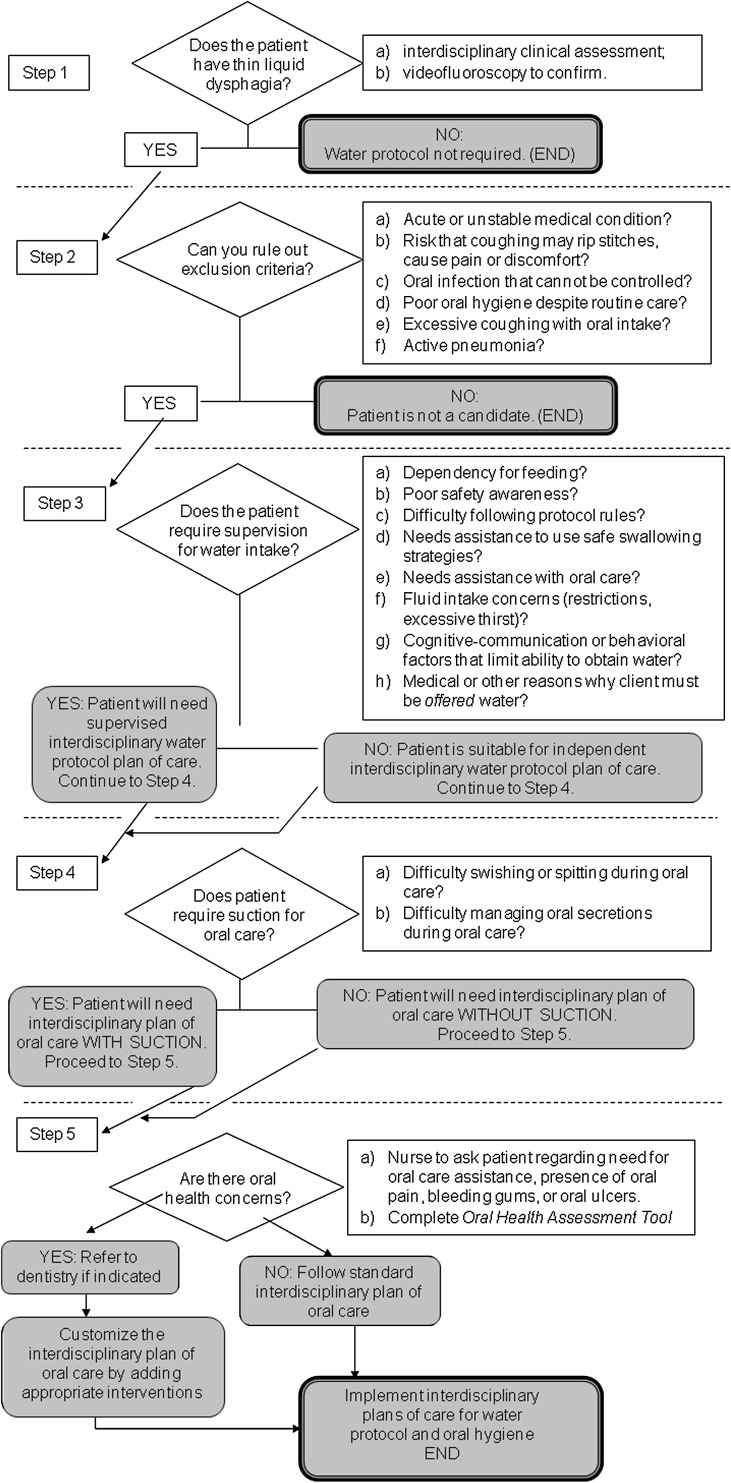
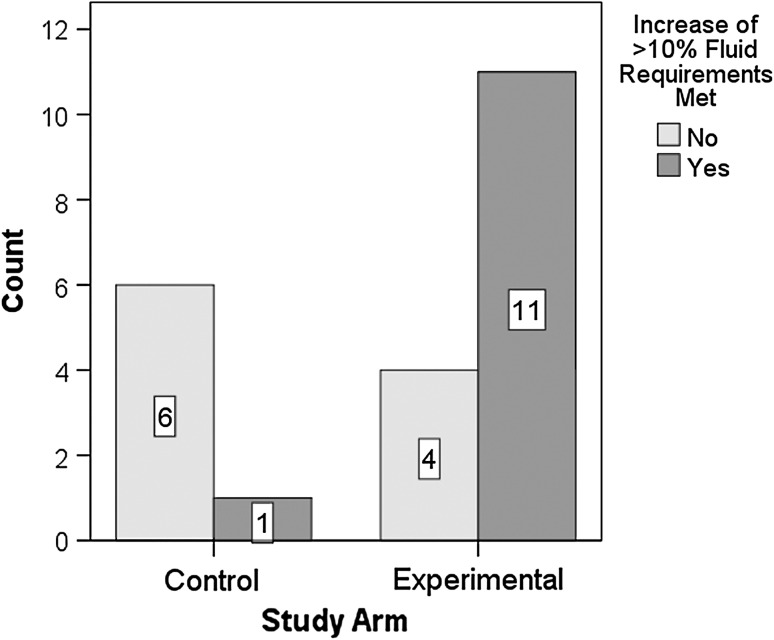
There is considerable clinical interest in the risks and benefits of offering oral water intake, in the form of water protocols, to patients with thin-liquid dysphagia. We describe the design and implementation of a water protocol for patients in a rehabilitation setting with videofluoroscopically confirmed thin-liquid aspiration. The GF Strong Water Protocol (GFSWP) is an interdisciplinary initiative, with roles and accountabilities specified for different members of the interprofessional health-care team. Rules of the water protocol specify mode of water access (independent, supervised), the implementation of any safe swallowing strategies recommended on the basis of the patient's videofluoroscopy, and procedures for evaluating and addressing oral care needs. Trial implementation of the water protocol in 15 participants showed that they remained free of adverse events, including pneumonia, over the course of an initial 14-day trial and continuing until discharge from the facility (range = 13-108 days). Seven participants were randomly assigned to a 14-day control phase in which they received standard care (without water access). Fluid intake measures taken after the oral water intake phase were increased (mean = 1,845 cc; 95% confidence interval: 1,520-2,169 cc) compared to those in the control phase (mean = 1,474 cc; 95% CI: 1,113-1,836 cc), with oral water intake measures comprising, on average, 563 cc (range = 238-888 cc) of the total post water trial fluid intake values. Fluid intake increased at least 10% of the calculated fluid requirements in 11/15 participants who received oral water access. These participants reported favorable quality-of-life outcomes, measured using the Swal-QOL. These findings support the implementation of the GFSWP, including its exclusion criteria, rules, and plans of care, for rehabilitation patients who aspirate thin liquids.
对于有稀薄液体吞咽困难的患者,提供口服水摄入(以水协议的形式)的风险和益处存在相当大的临床兴趣。我们描述了为在康复环境中经视频荧光透视证实有稀薄液体吸入的患者制定和实施水协议的设计和实施。GF Strong 水协议(GFSWP)是一项跨学科倡议,为跨专业医疗团队的不同成员指定了角色和责任。水协议规则规定了水的获取方式(独立、监督),根据患者的视频荧光透视结果实施任何安全吞咽策略,以及评估和解决口腔护理需求的程序。在 15 名参与者中试行水协议表明,在最初的 14 天试验期间以及在设施出院(范围为 13-108 天)期间,他们没有发生任何不良事件,包括肺炎。七名参与者被随机分配到为期 14 天的对照阶段,他们在该阶段接受标准护理(无口服水摄入)。与对照阶段相比(平均为 1,474cc;95%置信区间:1,113-1,836cc),在口服水摄入阶段后测量的液体摄入量增加(平均为 1,845cc;95%置信区间:1,520-2,169cc),并且口服水摄入措施平均占总水试验后液体摄入量的 563cc(范围为 238-888cc)。在接受口服水摄入的 15 名参与者中,有 11 名参与者的液体摄入量至少增加了计算出的液体需求的 10%。这些参与者报告了使用 Swal-QOL 测量的有利的生活质量结果。这些发现支持为有稀薄液体吸入的康复患者实施 GFSWP,包括其排除标准、规则和护理计划。