Division of General Internal Medicine, University of Pennsylvania, 423 Guardian Drive, Philadelphia, PA 19104, USA.
BMC Cardiovasc Disord. 2011 Sep 30;11:58. doi: 10.1186/1471-2261-11-58.
Reasons for race and gender differences in controlling elevated low density lipoprotein (LDL) cholesterol may be related to variations in prescribed lipid-lowering therapy. We examined the effect of lipid-lowering drug treatment and potency on time until LDL control for black and white women and men with a baseline elevated LDL.
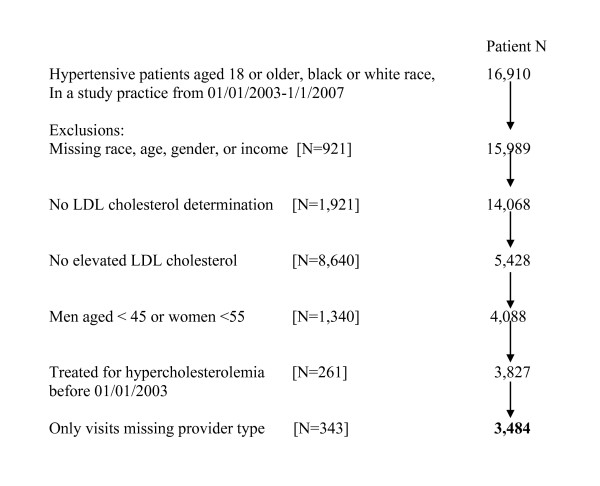
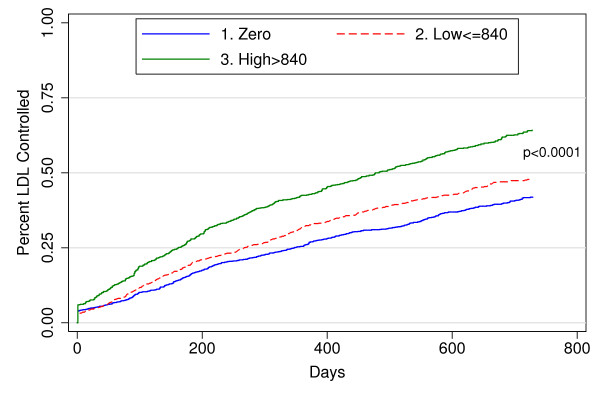
We studied 3,484 older hypertensive patients with dyslipidemia in 6 primary care practices over a 4-year timeframe. Potency of lipid-lowering drugs calculated for each treated day and summed to assess total potency for at least 6 and up to 24 months. Cox models of time to LDL control within two years and logistic regression models of control within 6 months by race-gender adjust for: demographics, clinical, health care delivery, primary/specialty care, LDL measurement, and drug potency.
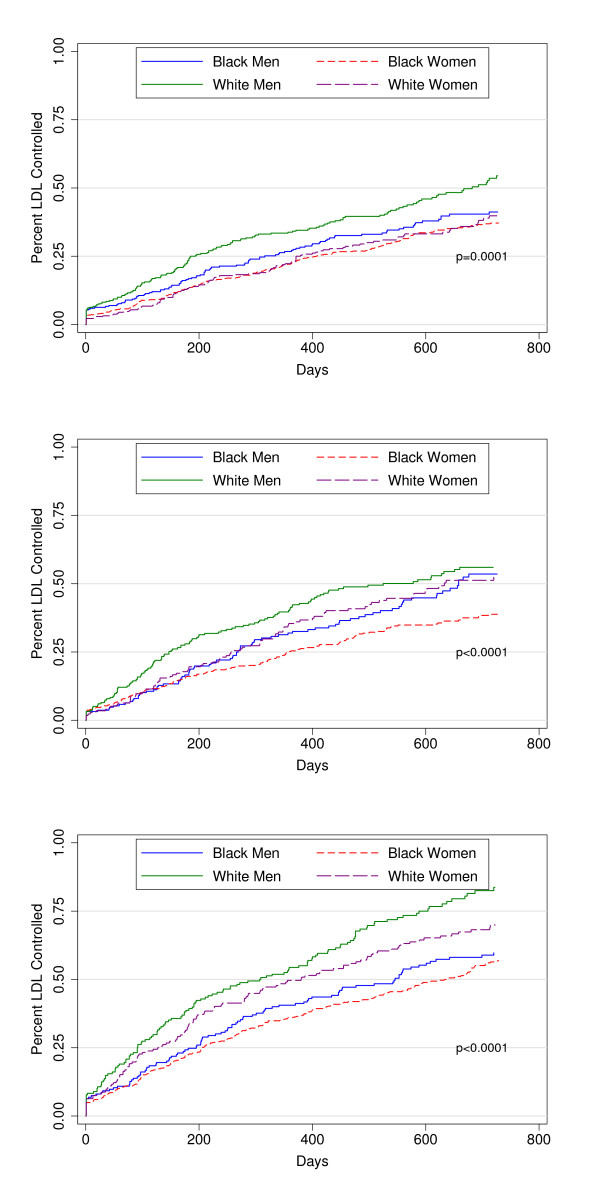
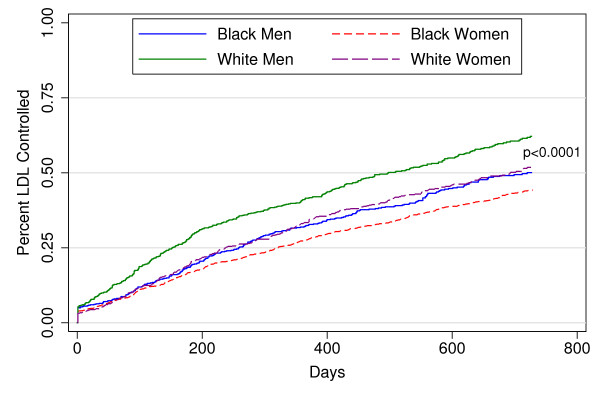
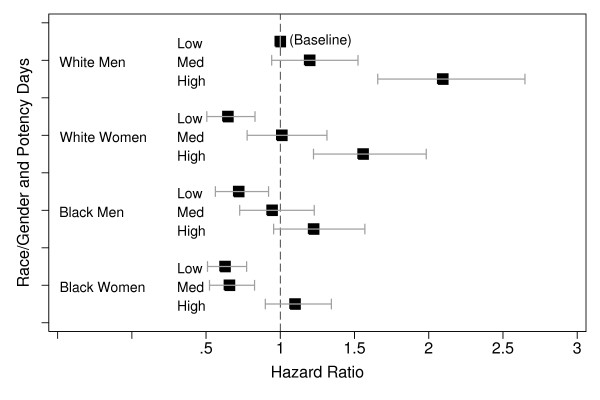
Time to LDL control decreased as lipid-lowering drug potency increased (P < 0.001). Black women (N = 1,440) received the highest potency therapy (P < 0.001) yet were less likely to achieve LDL control than white men (N = 717) (fully adjusted hazard ratio [HR] 0.66 [95% CI 0.56-0.78]). Black men (N = 666) and white women (N = 661) also had lower adjusted HRs of LDL control (0.82 [95% CI 0.69, 0.98] and 0.75 [95% CI 0.64-0.88], respectively) than white men. Logistic regression models of LDL control by 6 months and other sensitivity models affirmed these results.
Black women and, to a lesser extent, black men and white women were less likely to achieve LDL control than white men after accounting for lipid-lowering drug potency as well as diverse patient and provider factors. Future work should focus on the contributions of medication adherence and response to treatment to these clinically important differences.
控制升高的低密度脂蛋白(LDL)胆固醇的种族和性别差异的原因可能与规定的降脂治疗的变化有关。我们研究了降脂药物治疗和效力对基线升高 LDL 的黑人和白人女性和男性达到 LDL 控制的时间的影响。
我们在 4 年的时间里研究了 6 个初级保健实践中的 3484 名患有血脂异常的老年高血压患者。为每个治疗日计算降脂药物的效力,并将其相加,以评估至少 6 个月至 24 个月的总效力。在两年内达到 LDL 控制的时间的 Cox 模型和 6 个月内达到控制的逻辑回归模型按种族-性别调整:人口统计学、临床、医疗保健提供、初级/专业护理、LDL 测量和药物效力。
随着降脂药物效力的增加,达到 LDL 控制的时间减少(P < 0.001)。黑人女性(N = 1440)接受了最高效力的治疗(P < 0.001),但比白人男性(N = 717)更不可能达到 LDL 控制(完全调整后的危险比 [HR] 0.66 [95% CI 0.56-0.78])。黑人男性(N = 666)和白人女性(N = 661)的 LDL 控制调整后的 HR 也较低(0.82 [95% CI 0.69, 0.98]和 0.75 [95% CI 0.64-0.88])。6 个月时 LDL 控制的逻辑回归模型和其他敏感性模型证实了这些结果。
在考虑降脂药物效力以及不同的患者和提供者因素后,黑人女性,在较小程度上,黑人男性和白人女性比白人男性更不可能达到 LDL 控制。未来的工作应重点关注药物依从性和对治疗的反应对这些临床重要差异的贡献。