Department of Radiation Oncology, Memorial Sloan-Kettering Cancer Center, New York, NY, USA.
Int J Radiat Oncol Biol Phys. 2012 Apr 1;82(5):1816-22. doi: 10.1016/j.ijrobp.2011.02.057. Epub 2011 Sep 28.
Chloroma (granulocytic sarcoma) is a rare, extramedullary tumor of immature myeloid cells related to acute nonlymphocytic leukemia or myelodysplastic syndrome. Radiation therapy (RT) is often used in the treatment of chloromas; however, modern studies of RT are lacking. We reviewed our experience to analyze treatment response, disease control, and toxicity associated with RT to develop treatment algorithm recommendations for patients with chloroma.
Thirty-eight patients who underwent treatment for chloromas at our institution between February 1990 and June 2010 were identified and their medical records were reviewed and analyzed.
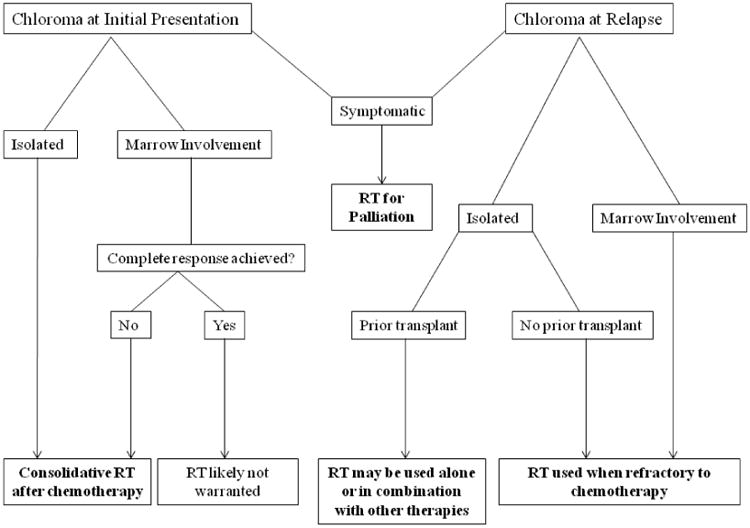
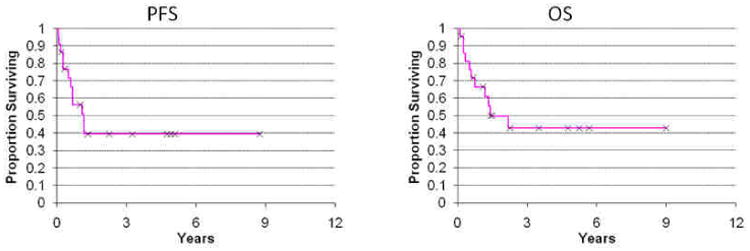
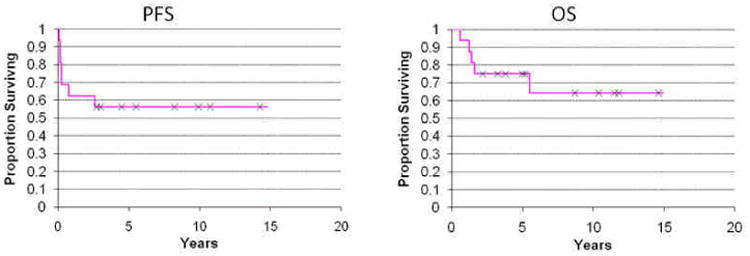
The majority of patients that presented with chloroma at the time of initial leukemia diagnosis (78%) have not received RT because it regressed after initial chemotherapy. Yet most patients that relapsed or remained with chloroma after chemotherapy are in the RT cohort (90%). Thirty-three courses of RT were administered to 22 patients. Radiation subsite breakdown was: 39% head and neck, 24% extremity, 9% spine, 9% brain, 6% genitourinary, 6% breast, 3% pelvis, and 3% genitourinary. Median dose was 20 (6-36) Gy. Kaplan-Meier estimates of progression-free survival and overall survival in the RT cohort were 39% and 43%, respectively, at 5 years. At a median follow-up of 11 months since RT, only 1 patient developed progressive disease at the irradiated site and 4 patients developed chloromas at other sites. RT was well tolerated without significant acute or late effects and provided symptom relief in 95% of cases.
The majority of patients with chloromas were referred for RT when there was extramedullary progression, marrow relapse, or rapid symptom relief required. RT resulted in excellent local disease control and palliation of symptoms without significant toxicity. We recommend irradiating chloromas to at least 20 Gy, and propose 24 Gy in 12 fractions as an appropriate regimen.
粒细胞肉瘤(绿色瘤)是一种罕见的、与急性非淋巴细胞白血病或骨髓增生异常综合征相关的未成熟髓系细胞的髓外肿瘤。放射治疗(RT)常用于治疗绿色瘤;然而,目前缺乏对 RT 的现代研究。我们回顾了我们的经验,以分析与 RT 相关的治疗反应、疾病控制和毒性,从而为患有绿色瘤的患者制定治疗方案建议。
我们确定了 1990 年 2 月至 2010 年 6 月期间在我们机构接受治疗的 38 名患有绿色瘤的患者,并对他们的病历进行了回顾和分析。
大多数在初始白血病诊断时出现绿色瘤的患者(78%)未接受 RT,因为它们在初始化疗后消退。然而,大多数在化疗后复发或仍有绿色瘤的患者都在 RT 组(90%)。22 名患者共接受了 33 次 RT。放射亚部位的细分是:39%的头颈部,24%的四肢,9%的脊柱,9%的脑部,6%的泌尿生殖系统,6%的乳房,3%的骨盆和 3%的泌尿生殖系统。中位剂量为 20(6-36)Gy。在 RT 组中,无进展生存期和总生存期的 Kaplan-Meier 估计值分别为 5 年时的 39%和 43%。在 RT 后中位随访 11 个月时,只有 1 例患者在照射部位出现进行性疾病,4 例患者在其他部位出现绿色瘤。RT 耐受性良好,无明显急性或迟发性毒性,并使 95%的病例症状缓解。
大多数患有绿色瘤的患者是在髓外进展、骨髓复发或需要快速缓解症状时被转介进行 RT。RT 可获得极佳的局部疾病控制和缓解症状,而无明显毒性。我们建议至少照射 20 Gy 的绿色瘤,并建议 24 Gy 分 12 次照射作为适当的方案。