Koletsis Efstratios N, Prokakis Christos, Crockett James R, Dedeilias Panagiotis, Panagiotou Matthew, Panagopoulos Nikolaos, Anastasiou Nikolaos, Dougenis Dimitrios, Apostolakis Efstratios
Cardiothoracic Surgery Department, University of Patras, School of Medicine, Patras, Greece.
J Cardiothorac Surg. 2011 Oct 3;6:127. doi: 10.1186/1749-8090-6-127.
Atrial fibrillation (AF) occurs in 28-33% of the patients undergoing coronary artery revascularization (CABG). This study focuses on both pre- and peri-operative factors that may affect the occurrence of AF. The aim is to identify those patients at higher risk to develop AF after CABG.
Two patient cohorts undergoing CABG were retrospectively studied. The first group (group A) consisted of 157 patients presenting AF after elective CABG. The second group (group B) consisted of 191 patients without AF postoperatively.
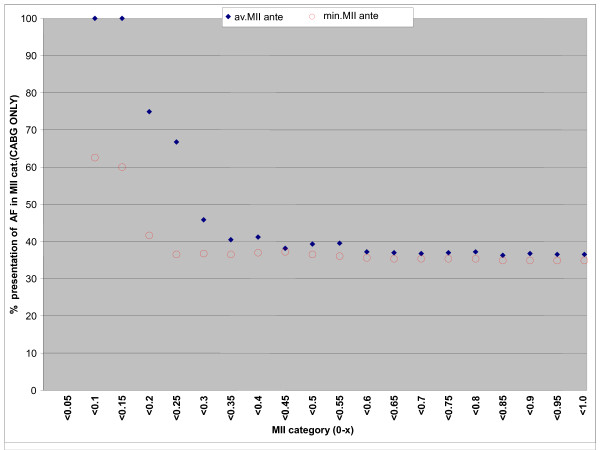
Preoperative factors presenting significant correlation with the incidence of post-operative AF included: 1) age > 65 years (p = 0.029), 2) history of AF (p = 0.022), 3) chronic obstructive pulmonary disease (p = 0.008), 4) left ventricular dysfunction with ejection fraction < 40% (p = 0.015) and 5) proximal lesion of the right coronary artery (p = 0.023). The intraoperative factors that appeared to have significant correlation with the occurrence of postoperative AF were: 1) CPB-time > 120 minutes (p = 0.011), 2) myocardial ischemia index < 0.27 ml.m2/Kg.min (p = 0.011), 3) total positive fluid-balance during ICU-stay (p < 0.001), 4) FiO2/PO2 > 0, 4 after extubation and during the ICU-stay (p = 0.021), 5) inotropic support with doses 15-30 μg/Kg/min (p = 0.016), 6) long ICU-stay recovery for any reason (p < 0.001) and perioperative myocardial infarction (p < 0.001).
Our results suggest that the incidence of post-CABG atrial fibrillation can be predicted by specific preoperative and intraoperative measures. The intraoperative myocardial ischemia can be sufficiently quantified by the myocardial ischemia index. For those patients at risk we would suggest an early postoperative precautionary anti-arrhythmic treatment.
在接受冠状动脉血运重建术(CABG)的患者中,心房颤动(AF)的发生率为28%-33%。本研究聚焦于可能影响AF发生的术前和围手术期因素。目的是识别CABG术后发生AF风险较高的患者。
对两组接受CABG的患者进行回顾性研究。第一组(A组)由157例择期CABG术后出现AF的患者组成。第二组(B组)由191例术后未发生AF的患者组成。
与术后AF发生率显著相关的术前因素包括:1)年龄>65岁(p = 0.029),2)AF病史(p = 0.022),3)慢性阻塞性肺疾病(p = 0.008),4)左心室功能障碍,射血分数<40%(p = 0.015),5)右冠状动脉近端病变(p = 0.023)。与术后AF发生似乎显著相关的术中因素为:1)体外循环时间>120分钟(p = 0.011),2)心肌缺血指数<0.27 ml.m2/Kg.min(p = 0.011),3)重症监护病房(ICU)住院期间总液体正平衡(p<0.001),4)拔管后及ICU住院期间FiO2/PO2>0.4(p = 0.021),5)剂量为15-30μg/Kg/min的血管活性药物支持(p = 0.016),6)因任何原因在ICU长时间恢复(p<0.001)及围手术期心肌梗死(p<0.001)。
我们的结果表明,CABG术后心房颤动的发生率可通过特定的术前和术中措施进行预测。术中心肌缺血可通过心肌缺血指数进行充分量化。对于那些有风险的患者,我们建议术后尽早进行预防性抗心律失常治疗。