Department of Emergency Medicine, NYU School of Medicine, 462 First Avenue, New York, NY 10016, USA.
BMC Health Serv Res. 2011 Oct 13;11:270. doi: 10.1186/1472-6963-11-270.
A small percentage of high-risk patients accounts for a large proportion of Medicaid spending in the United States, which has become an urgent policy issue. Our objective was to pilot a novel patient-centered intervention for high-risk patients with frequent hospital admissions to determine its potential to improve care and reduce costs.
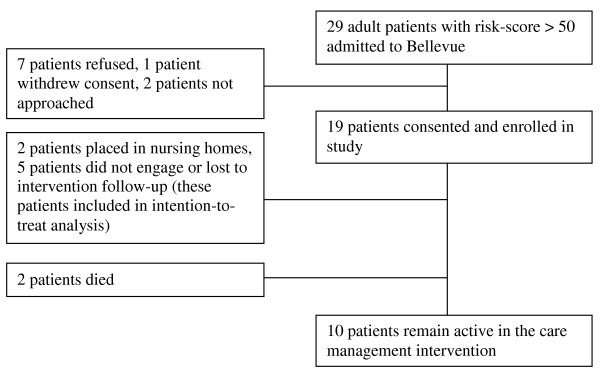
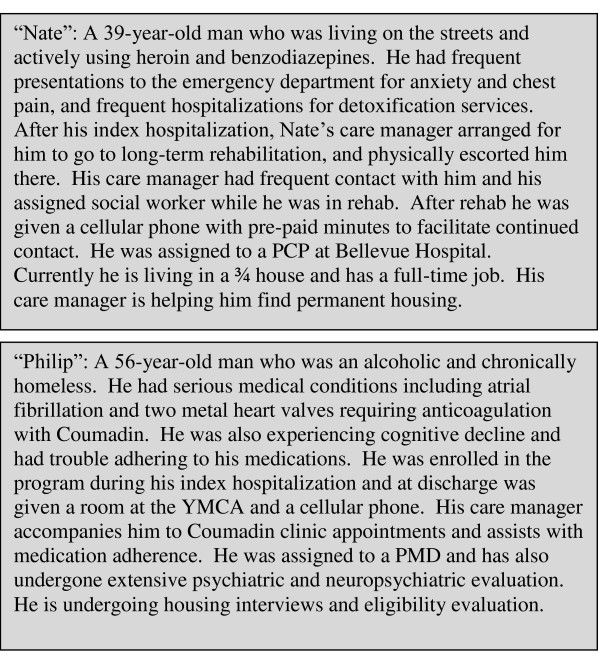
Community and hospital-based care management and coordination intervention with pre-post analysis of health care utilization. We enrolled Medicaid fee-for-service patients aged 18-64 who were admitted to an urban public hospital and identified as being at high risk for hospital readmission by a validated predictive algorithm. Enrolled patients were evaluated using qualitative and quantitative interview techniques to identify needs such as transportation to/advocacy during medical appointments, mental health/substance use treatment, and home visits. A community housing partner initiated housing applications in-hospital for homeless patients. Care managers facilitated appropriate discharge plans then worked closely with patients in the community using a harm reduction approach.
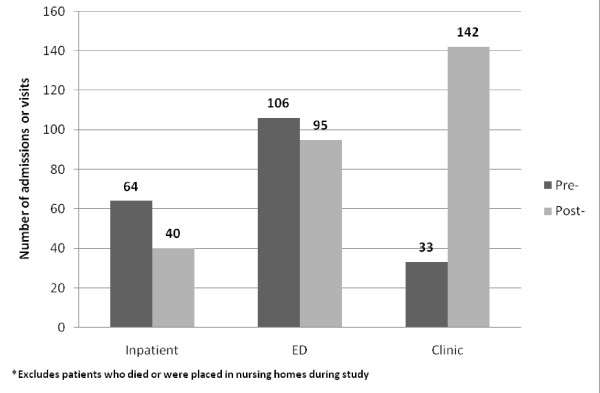
Nineteen patients were enrolled; all were male, 18/19 were substance users, and 17/19 were homeless. Patients had a total of 64 inpatient admissions in the 12 months before the intervention, versus 40 in the following 12 months, a 37.5% reduction. Most patients (73.3%) had fewer inpatient admissions in the year after the intervention compared to the prior year. Overall ED visits also decreased after study enrollment, while outpatient clinic visits increased. Yearly study hospital Medicaid reimbursements fell an average of $16,383 per patient.
A pilot intervention for high-cost patients shows promising results for health services usage. We are currently expanding our model to serve more patients at additional hospitals to see if the pilot's success can be replicated.
Clinicaltrials.gov Identifier: NCT01292096.
在美国,一小部分高风险患者的医疗支出占医疗补助计划(Medicaid)支出的很大比例,这已成为一个紧迫的政策问题。我们的目标是为频繁住院的高风险患者试点一种新的以患者为中心的干预措施,以确定其改善护理和降低成本的潜力。
采用社区和医院为基础的护理管理和协调干预措施,对医疗保健利用情况进行前后分析。我们招募了年龄在 18-64 岁之间的医疗补助计划按服务收费患者,这些患者在城市公立医院住院,并通过经过验证的预测算法被确定为有再次住院的高风险。通过定性和定量访谈技术评估入组患者,以确定他们的需求,如就医交通/代理、心理健康/药物使用治疗和家访。社区住房合作伙伴在医院为无家可归的患者发起住房申请。护理经理协助制定适当的出院计划,然后使用减少伤害的方法在社区中与患者密切合作。
共招募了 19 名患者;他们都是男性,18/19 名是药物使用者,17/19 名是无家可归者。在干预前的 12 个月中,患者总共住院 64 次,而在接下来的 12 个月中,住院次数减少到 40 次,减少了 37.5%。与前一年相比,大多数患者(73.3%)在干预后的一年中住院次数减少。研究入组后,急诊就诊次数总体减少,而门诊就诊次数增加。每位患者的年度研究医院医疗补助计划报销费用平均减少 16,383 美元。
针对高成本患者的试点干预措施在医疗服务使用方面显示出有希望的结果。我们目前正在扩大我们的模式,为更多的患者提供服务,在其他医院进行服务,以确定试点的成功是否可以复制。
Clinicaltrials.gov 标识符:NCT01292096。