Division of Research, Kaiser Permanente Northern California, Oakland.
JAMA Netw Open. 2024 Sep 3;7(9):e2435199. doi: 10.1001/jamanetworkopen.2024.35199.
Integrated health care systems have initiated major investments to identify and address social risks, particularly for patients with multiple medical conditions.
To evaluate the association of social risks with health care use among patients with complex multimorbidity.
DESIGN, SETTING, AND PARTICIPANTS: This longitudinal cohort study assessed Kaiser Permanente Northern California (KPNC) patients with (1) moderate medical complexity (defined by high comorbidity score, high risk of hospitalization, and/or prior emergency department [ED] admissions) and (2) high medical complexity (eg, meeting additional criteria, such as ≥7 medications and laboratory evidence of poor disease control).
Social risks (eg, requiring medical financial assistance and self-reported social barriers to care).
Inpatient and outpatient health care use during 12 months of follow-up (January 15, 2023, to January 14, 2024).
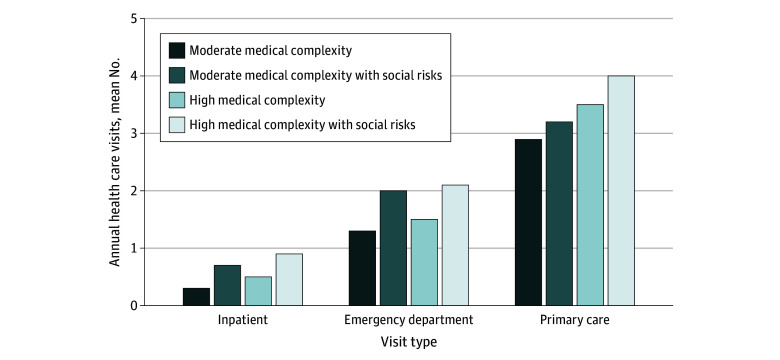
The sample included 97 252 KPNC patients (mean [SD] age, 69.5 [16] years; 52.1% female; 10.6% Asian, 11.1% Black, 18.3% Hispanic, 54.6% White, and 5.5% other race or ethnicity [eg, American Indian or Alaskan Native, Native Hawaiian or Pacific Islander, multiracial, or unknown race]; and 8.8% insured by Medicaid), including 27 827 with moderate medical complexity (5074 [18.2%] with social risks) and 69 425 with high medical complexity (17 343 [25.0%] with social risks). In fully adjusted models, for moderate medical complexity, social risks were associated with higher odds of inpatient admissions (odds ratio [OR], 1.2; 95% CI, 1.1-1.4), ED visits (OR, 1.2; 95% CI, 1.1-1.3), and mental health visits (OR, 1.2; 95% CI, 1.1-1.3) vs individuals without social risks. Among individuals with high medical complexity, social risks were associated with higher odds of inpatient admissions (OR, 1.2; 95% CI, 1.1-1.2), ED visits (OR, 1.2; 95% CI, 1.1-1.2), and 30-day readmissions (OR, 1.2; 95% CI, 1.1-1.3) and higher odds of mental health visits (OR, 1.3; 95% CI, 1.2-1.3) vs individuals without social risks.
In this cohort study of individuals with medical complexity, coexisting social risks were associated with substantial downstream health care use. Efforts to reduce use in individuals with complex medical comorbidity could include concurrent efforts to identify and reduce social risks.
综合医疗保健系统已投入大量资金来识别和解决社会风险,特别是针对患有多种疾病的患者。
评估社会风险与患有复杂多重疾病的患者的医疗保健使用之间的关联。
设计、设置和参与者:这项纵向队列研究评估了 Kaiser Permanente Northern California(KPNC)的患者(1)中度医疗复杂性(定义为高合并症评分、高住院风险和/或先前急诊部[ED]就诊)和(2)高医疗复杂性(例如,满足其他标准,如≥7 种药物和疾病控制不良的实验室证据)。
社会风险(例如,需要医疗财政援助和自我报告的护理障碍)。
在 12 个月的随访期间(2023 年 1 月 15 日至 2024 年 1 月 14 日)的住院和门诊医疗保健使用情况。
样本包括 97252 名 KPNC 患者(平均[标准差]年龄,69.5[16]岁;52.1%女性;10.6%亚裔,11.1%黑人,18.3%西班牙裔,54.6%白人,5.5%其他种族或民族[例如,美洲印第安人或阿拉斯加原住民、夏威夷原住民或太平洋岛民、多种族或未知种族];18.3%的人由医疗补助保险承保),包括 27827 名中度医疗复杂性患者(5074 名[18.2%]有社会风险)和 69425 名高度医疗复杂性患者(17343 名[25.0%]有社会风险)。在完全调整的模型中,对于中度医疗复杂性,社会风险与住院入院(优势比[OR],1.2;95%置信区间[CI],1.1-1.4)、急诊就诊(OR,1.2;95%CI,1.1-1.3)和心理健康就诊(OR,1.2;95%CI,1.1-1.3)的可能性更高,而不是没有社会风险的个体。在具有高度医疗复杂性的个体中,社会风险与住院入院(OR,1.2;95%CI,1.1-1.2)、急诊就诊(OR,1.2;95%CI,1.1-1.2)和 30 天再入院(OR,1.2;95%CI,1.1-1.3)以及心理健康就诊(OR,1.3;95%CI,1.2-1.3)的可能性更高,而不是没有社会风险的个体。
在这项针对患有医疗复杂性的个体的队列研究中,并存的社会风险与大量下游医疗保健使用相关。减少患有复杂合并症的个体医疗使用的努力可能包括同时努力识别和减少社会风险。