National Heart, Lung and Blood Institute's Framingham Heart Study and Center for Population Studies, Framingham, MA 01702, USA.
Am J Kidney Dis. 2012 Jan;59(1):19-24. doi: 10.1053/j.ajkd.2011.08.030. Epub 2011 Oct 13.
Recent genome-wide association studies have identified multiple genetic loci that increase the risk of chronic kidney disease (CKD) in the general population. We hypothesized that knowledge of these loci might permit improved CKD risk prediction beyond that provided by traditional phenotypic risk factors.
Observational cohort study.
SETTING & PARTICIPANTS: Participants who attended the 15th (1977-1979) and 24th (1995-1998) examination cycles of the original cohort or the 6th (1995-1998) and 8th cycles (2005-2008) of the offspring cohort of the Framingham Heart Study (n = 2,489).
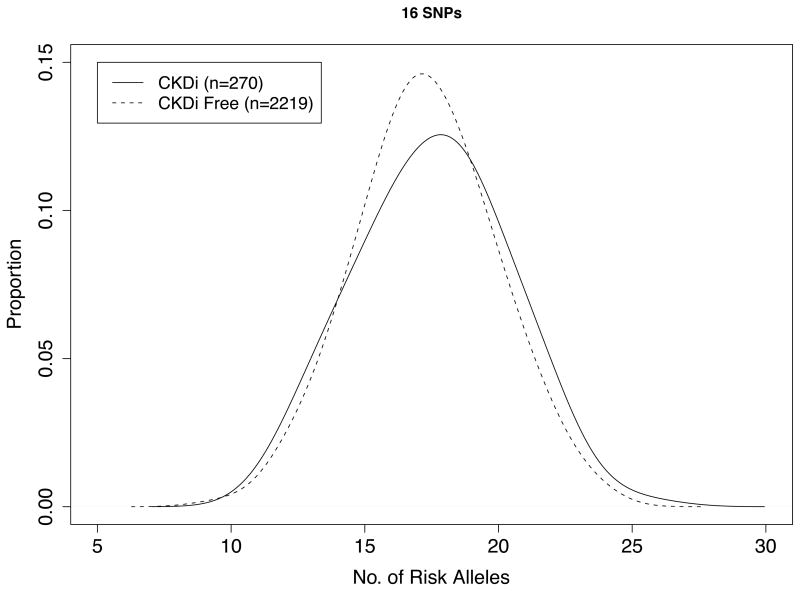
Single-nucleotide polymorphisms at 16 stage 3 CKD loci were genotyped and used to construct a genetic risk score. Standard clinical predictors of incident stage 3 CKD also were used.
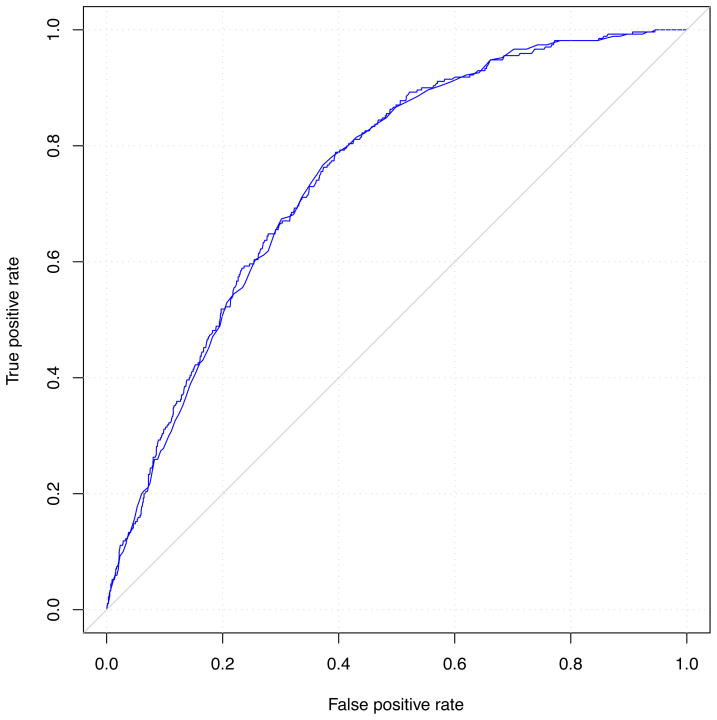
OUTCOMES & MEASUREMENTS: Incident stage 3 CKD was defined as estimated glomerular filtration rate <60 mL/min/1.73 m(2) at follow-up. Participants with baseline stage 3 CKD were excluded. Logistic regression was used to generate C statistics, which measured the power of the genetic risk score to discriminate risk of incident CKD stage 3 with and without traditional risk factors.
There were 270 new stage 3 CKD cases during an average of 10.8 years of follow-up. Mean genetic risk score was 17.5 ± 2.8 (SD) for those who developed stage 3 CKD and 17.3 ± 2.6 for those who did not (P for genotype score difference = 0.2). The OR for stage 3 CKD was 1.06 (95% CI, 1.01-1.11; P = 0.03) per additional risk allele, adjusting for age and sex. In the age- and sex-adjusted model, the C statistic was 0.748 without the genotype score and 0.751 with the score (P difference = 0.3). The risk score was not statistically significant in a multivariable model adjusted for standard stage 3 CKD risk factors (P = 0.07).
All participants were of European ancestry; the genotype score may not be valid in different ancestral groups.
A genetic score generated from 16 known CKD risk alleles did not predict new cases of stage 3 CKD in the community beyond knowledge of common clinical risk factors alone.
最近的全基因组关联研究已经确定了多个增加普通人群慢性肾脏病(CKD)风险的遗传位点。我们假设,这些位点的知识可能会允许对 CKD 风险的预测进行改进,超过传统表型风险因素所提供的预测。
观察性队列研究。
参加弗雷明汉心脏研究原始队列第 15 次(1977-1979 年)和第 24 次(1995-1998 年)检查周期或后代队列第 6 次(1995-1998 年)和第 8 次周期(2005-2008 年)的参与者(n=2489)。
16 个 CKD 第 3 期的单核苷酸多态性进行基因分型,并用于构建遗传风险评分。还使用了预测 CKD 第 3 期的标准临床预测因素。
新发 CKD 第 3 期的定义为随访时估算肾小球滤过率 <60 mL/min/1.73 m(2)。排除了基线 CKD 第 3 期的参与者。使用逻辑回归生成 C 统计量,该统计量衡量遗传风险评分与不考虑传统危险因素的情况下,预测 CKD 第 3 期风险的能力。
在平均 10.8 年的随访中,有 270 例新发生的 CKD 第 3 期病例。发生 CKD 第 3 期的患者的平均遗传风险评分为 17.5±2.8(SD),未发生 CKD 第 3 期的患者为 17.3±2.6(P 基因型评分差异=0.2)。每个额外的风险等位基因的 CKD 第 3 期的 OR 为 1.06(95%CI,1.01-1.11;P=0.03),调整年龄和性别。在年龄和性别调整模型中,无基因型评分时的 C 统计量为 0.748,有评分时为 0.751(P 差值=0.3)。在调整了标准 CKD 第 3 期风险因素的多变量模型中,风险评分没有统计学意义(P=0.07)。
所有参与者均为欧洲血统;基因型评分在不同的祖先群体中可能无效。
由 16 个已知的 CKD 风险等位基因生成的遗传评分不能在社区中新发 CKD 第 3 期病例中预测,超过仅基于常见临床风险因素的知识。