Department of Medicine, Division of Hematology/Oncology, UPMC, University of Pittsburgh Cancer Institute, 300 Halket Street, Suite 4628, Pittsburgh, PA 15213, USA.
Breast Cancer Res. 2011 Oct 14;13(5):R98. doi: 10.1186/bcr3038.
Breast Cancer Index (BCI) combines two independent biomarkers, HOXB13:IL17BR (H:I) and the 5-gene molecular grade index (MGI), that assess estrogen-mediated signalling and tumor grade, respectively. BCI stratifies early-stage estrogen-receptor positive (ER+), lymph-node negative (LN-) breast cancer patients into three risk groups and provides a continuous assessment of individual risk of distant recurrence. Objectives of the current study were to validate BCI in a clinical case series and to compare the prognostic utility of BCI and Adjuvant!Online (AO).
Tumor samples from 265 ER+LN- tamoxifen-treated patients were identified from a single academic institution's cancer research registry. The BCI assay was performed and scores were assigned based on a pre-determined risk model. Risk was assessed by BCI and AO and correlated to clinical outcomes in the patient cohort.
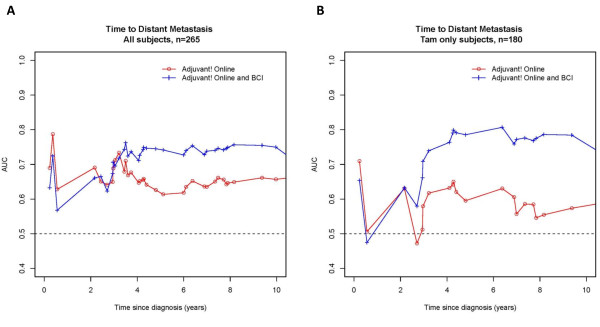
BCI was a significant predictor of outcome in a cohort of 265 ER+LN- patients (median age: 56-y; median follow-up: 10.3-y), treated with adjuvant tamoxifen alone or tamoxifen with chemotherapy (32%). BCI categorized 55%, 21%, and 24% of patients as low, intermediate and high-risk, respectively. The 10-year rates of distant recurrence were 6.6%, 12.1% and 31.9% and of breast cancer-specific mortality were 3.8%, 3.6% and 22.1% in low, intermediate, and high-risk groups, respectively. In a multivariate analysis including clinicopathological factors, BCI was a significant predictor of distant recurrence (HR for 5-unit increase = 5.32 [CI 2.18-13.01; P = 0.0002]) and breast cancer-specific mortality (HR for a 5-unit increase = 9.60 [CI 3.20-28.80; P < 0.0001]). AO was significantly associated with risk of recurrence. In a separate multivariate analysis, both BCI and AO were significantly predictive of outcome. In a time-dependent (10-y) ROC curve accuracy analysis of recurrence risk, the addition of BCI+AO increased predictive accuracy in all patients from 66% (AO only) to 76% (AO+BCI) and in tamoxifen-only treated patients from 65% to 81%.
This study validates the prognostic performance of BCI in ER+LN- patients. In this characteristically low-risk cohort, BCI classified high versus low-risk groups with ~5-fold difference in 10-year risk of distant recurrence and breast cancer-specific death. BCI and AO are independent predictors with BCI having additive utility beyond standard of care parameters that are encompassed in AO.
乳腺癌指数(BCI)结合了两个独立的生物标志物,HOXB13:IL17BR(H:I)和 5 基因分子分级指数(MGI),分别评估雌激素介导的信号和肿瘤分级。BCI 将早期雌激素受体阳性(ER+)、淋巴结阴性(LN-)乳腺癌患者分为三个风险组,并对个体远处复发的风险进行连续评估。本研究的目的是在临床病例系列中验证 BCI,并比较 BCI 和 Adjuvant!Online(AO)的预后效用。
从一家学术机构的癌症研究登记处确定了 265 例接受他莫昔芬治疗的 ER+LN-患者的肿瘤样本。进行了 BCI 检测,并根据预先确定的风险模型分配了评分。通过 BCI 和 AO 评估风险,并与患者队列的临床结果相关联。
BCI 是 265 例 ER+LN-患者(中位年龄:56 岁;中位随访:10.3 年)队列中结局的显著预测因子,这些患者单独接受辅助他莫昔芬或他莫昔芬联合化疗(32%)治疗。BCI 将 55%、21%和 24%的患者分别归类为低、中、高风险组。低、中、高风险组 10 年远处复发率分别为 6.6%、12.1%和 31.9%,乳腺癌特异性死亡率分别为 3.8%、3.6%和 22.1%。在包括临床病理因素的多变量分析中,BCI 是远处复发的显著预测因子(5 个单位增加的 HR = 5.32[CI 2.18-13.01;P = 0.0002])和乳腺癌特异性死亡率(5 个单位增加的 HR = 9.60[CI 3.20-28.80;P < 0.0001])。AO 与复发风险显著相关。在单独的多变量分析中,BCI 和 AO 均与结局显著相关。在复发风险的时间依赖性(10 年)ROC 曲线准确性分析中,在所有患者中,BCI+AO 的添加将预测准确性从 66%(仅 AO)提高到 76%(BCI+AO),在仅接受他莫昔芬治疗的患者中从 65%提高到 81%。
本研究验证了 BCI 在 ER+LN-患者中的预后性能。在这个典型的低风险队列中,BCI 将高风险组与低风险组区分开来,10 年远处复发和乳腺癌特异性死亡的风险差异约为 5 倍。BCI 和 AO 是独立的预测因子,BCI 在包含在 AO 中的标准治疗参数之外具有附加效用。