Department of Physiology and Pharmacology, University of Western Ontario, London, ON, Canada.
J Pain Res. 2011;4:315-23. doi: 10.2147/JPR.S17882. Epub 2011 Sep 29.
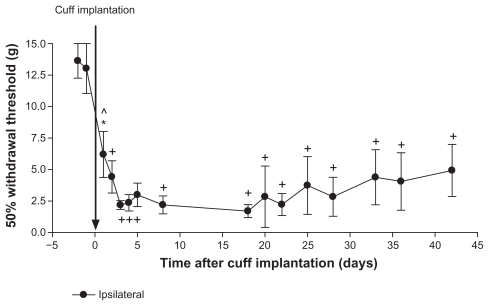
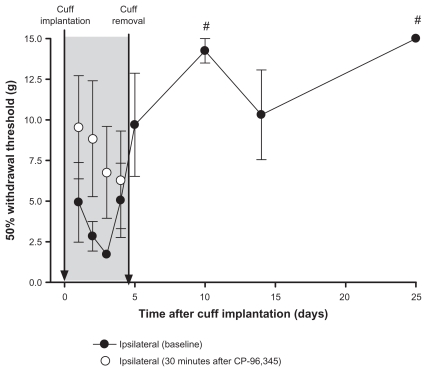
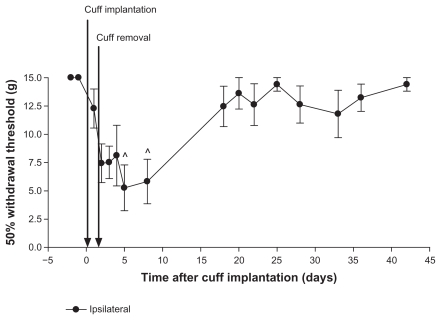
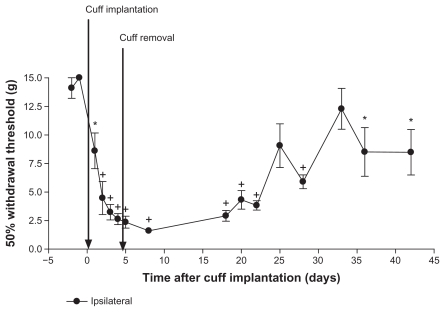
Peripheral neuropathic pain arises from trauma to sensory nerves. Other types of acute neurotrauma such as stroke and spinal cord injury are treated immediately, largely to prevent secondary damage. To pursue the possibility that neuropathic pain may also be amenable to early treatment, a rat model of neuropathic pain was induced using a 2-mm polyethylene cuff implanted around one sciatic nerve. Within 24 hours, hypersensitivity to von Frey hair stimulation appeared, as indicated by decreased paw withdrawal thresholds. When the cuff was removed 24 hours after implantation, readings returned to pre-implantation levels starting as early as day 18. When the cuff was removed after 4 days, there was a period of initial hypersensitivity, and then an increase toward baseline at two time points near the end of the study; therefore, only a partial recovery toward pre-implantation values occurred. Having established that a temporal reversal can occur, the next step examined possible pharmacological reversal. The tachykinin NK(1) receptor antagonist, CP-96,345, produced a minor increase in withdrawal thresholds in animals with the cuff left permanently implanted. To determine the effect of early and repeated administration of CP-96,345, it was given daily on days 1-4. The cuff was removed on day 4. Six days later, readings showed reversal of tactile hypersensitivity. We suggest that persistent neuropathic pain occurs from processes that develop over several hours and days, and that some of these processes may be prevented by early medical intervention. Thus, nerve injury in the context of chronic neuropathic pain should be treated in a similar manner to nerve injury resulting from stroke, spinal cord injury, and other types of neurotrauma. We suggest that effective medical intervention within the first few hours after nerve injury may spare a patient from a chronic debilitating pain that may be refractory to later therapies.
周围神经病理性疼痛源于感觉神经损伤。其他类型的急性神经创伤,如中风和脊髓损伤,会立即进行治疗,主要是为了防止继发损伤。为了探索神经病理性疼痛也可能适合早期治疗的可能性,研究人员使用植入大鼠一只坐骨神经周围的 2 毫米聚乙烯袖套建立了神经病理性疼痛模型。在 24 小时内,对 von Frey 毛发刺激的敏感性增加,表现为爪回缩阈值降低。植入后 24 小时去除袖套时,读数在植入前水平开始,最早在第 18 天恢复。在第 4 天去除袖套后,有一个初始超敏反应期,然后在研究结束时的两个时间点向基线增加;因此,只有部分恢复到植入前的值。研究人员已经证实可以发生时间逆转,下一步研究了可能的药物逆转。速激肽 NK(1)受体拮抗剂 CP-96,345 在永久性植入袖套的动物中,轻微增加了退缩阈值。为了确定 CP-96,345 早期和重复给药的效果,在第 1-4 天每天给予 CP-96,345。第 4 天去除袖套。六天后,读数显示触觉过敏逆转。研究人员认为,持续性神经病理性疼痛是由数小时和数天发展而来的过程引起的,这些过程中的一些可能可以通过早期的医学干预来预防。因此,慢性神经病理性疼痛背景下的神经损伤应该以类似于中风、脊髓损伤和其他类型的神经创伤导致的神经损伤的方式进行治疗。研究人员认为,在神经损伤后的最初几个小时内进行有效的医学干预可能会使患者免受可能对后期治疗产生抗药性的慢性衰弱性疼痛的困扰。