Division of Cardiovascular Medicine, Department of Medicine, Brigham & Women's Hospital, Boston, MA 02115, USA.
Circulation. 2011 Nov 15;124(20):2215-24. doi: 10.1161/CIRCULATIONAHA.111.050427. Epub 2011 Oct 17.
Impaired vasodilator function is an early manifestation of coronary artery disease and may precede angiographic stenosis. It is unknown whether noninvasive assessment of coronary vasodilator function in patients with suspected or known coronary artery disease carries incremental prognostic significance.
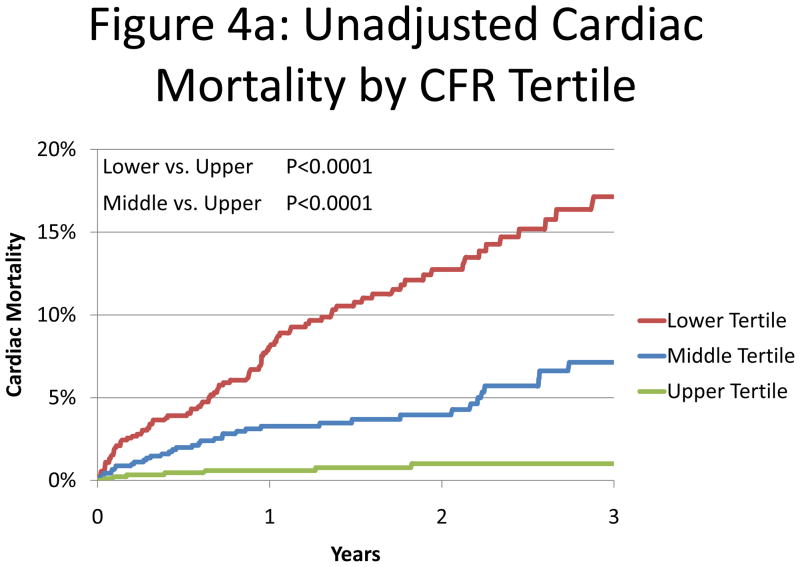
A total of 2783 consecutive patients referred for rest/stress positron emission tomography were followed up for a median of 1.4 years (interquartile range, 0.7-3.2 years). The extent and severity of perfusion abnormalities were quantified by visual evaluation of myocardial perfusion images. Rest and stress myocardial blood flows were calculated with factor analysis and a 2-compartment kinetic model and were used to compute coronary flow reserve (coronary flow reserve equals stress divided by rest myocardial blood flow). The primary end point was cardiac death. Overall 3-year cardiac mortality was 8.0%. The lowest tertile of coronary flow reserve (<1.5) was associated with a 5.6-fold increase in the risk of cardiac death (95% confidence interval, 2.5-12.4; P<0.0001) compared with the highest tertile. Incorporation of coronary flow reserve into cardiac death risk assessment models resulted in an increase in the c index from 0.82 (95% confidence interval, 0.78-0.86) to 0.84 (95% confidence interval, 0.80-0.87; P=0.02) and in a net reclassification improvement of 0.098 (95% confidence interval, 0.025-0.180). Addition of coronary flow reserve resulted in correct reclassification of 34.8% of intermediate-risk patients (net reclassification improvement=0.487; 95% confidence interval, 0.262-0.731). Corresponding improvements in risk assessment for mortality from any cause were also demonstrated.
Noninvasive quantitative assessment of coronary vasodilator function with positron emission tomography is a powerful, independent predictor of cardiac mortality in patients with known or suspected coronary artery disease and provides meaningful incremental risk stratification over clinical and gated myocardial perfusion imaging variables.
血管舒张功能受损是冠状动脉疾病的早期表现,可能先于血管造影狭窄。目前尚不清楚在疑似或已知患有冠状动脉疾病的患者中,非侵入性冠状动脉舒张功能评估是否具有额外的预后意义。
对 2783 例连续就诊的行静息/负荷正电子发射断层扫描的患者进行了中位时间为 1.4 年(四分位间距为 0.7-3.2 年)的随访。通过心肌灌注图像的视觉评估量化灌注异常的程度和严重程度。采用因子分析和双室动力学模型计算静息和负荷状态下的心肌血流,并计算冠状动脉血流储备(冠状动脉血流储备=负荷/静息心肌血流)。主要终点为心脏性死亡。总体 3 年心脏死亡率为 8.0%。冠状动脉血流储备最低三分位组(<1.5)与心脏性死亡风险增加 5.6 倍相关(95%置信区间,2.5-12.4;P<0.0001),与最高三分位组相比。将冠状动脉血流储备纳入心脏死亡风险评估模型可使 c 指数从 0.82(95%置信区间,0.78-0.86)增加到 0.84(95%置信区间,0.80-0.87;P=0.02),净重新分类改善为 0.098(95%置信区间,0.025-0.180)。冠状动脉血流储备可正确重新分类 34.8%的中度风险患者(净重新分类改善=0.487;95%置信区间,0.262-0.731)。还证明了对任何原因导致的死亡率进行风险评估的改善。
正电子发射断层扫描的冠状动脉舒张功能无创定量评估是已知或疑似冠状动脉疾病患者心脏死亡率的有力、独立预测指标,与临床和门控心肌灌注成像变量相比,可提供有意义的增量危险分层。