PHDC Masters Programme, London School of Hygiene & Tropical Medicine, UK.
Hum Resour Health. 2011 Oct 24;9:27. doi: 10.1186/1478-4491-9-27.
Over thirty years have passed since the Alma-Ata Declaration on primary health care in 1978. Many governments in the first decade following the declaration responded by developing national programmes of community health workers (CHWs), but evaluations of these often demonstrated poor outcomes. As many CHW programmes have responded to the HIV/AIDS pandemic, international interest in them has returned and their role in the response to other diseases should be examined carefully so that lessons can be applied to their new roles. Over half of the deaths in African children under five years of age are due to malaria, diarrhoea and pneumonia - a situation which could be addressed through the use of cheap and effective interventions delivered by CHWs. However, to date there is very little evidence from randomised controlled trials of the impacts of CHW programmes on child mortality in Africa. Evidence from non-randomised controlled studies has not previously been reviewed systematically.
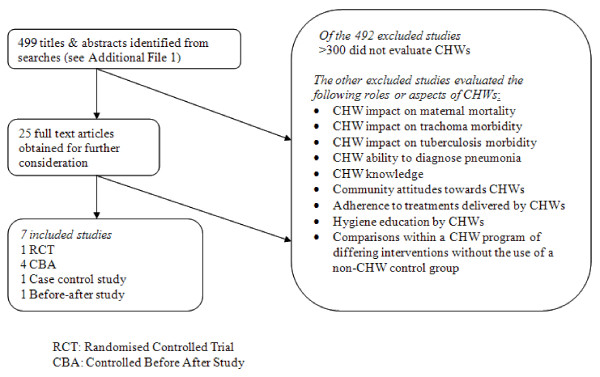
We searched databases of published and unpublished studies for RCTs and non-randomised studies evaluating CHW programmes delivering curative treatments, with or without preventive components, for malaria, diarrhoea or pneumonia, in children in sub-Saharan Africa from 1987 to 2007. The impact of these programmes on morbidity or mortality in children under six years of age was reviewed. A descriptive analysis of interventional and contextual factors associated with these impacts was attempted.
The review identified seven studies evaluating CHWs, delivering a range of interventions. Limited descriptive data on programmes, contexts or process outcomes for these CHW programmes were available. CHWs in national programmes achieved large mortality reductions of 63% and 36% respectively, when insecticide-treated nets and anti-malarial chemoprophylaxis were delivered, in addition to curative interventions.
CHW programmes could potentially achieve large gains in child survival in sub-Saharan Africa if these programmes were implemented at scale. Large-scale rigorous studies, including RCTs, are urgently needed to provide policymakers with more evidence on the effects of CHWs delivering these interventions.
自 1978 年《阿拉木图初级卫生保健宣言》发布以来,已经过去了三十多年。宣言发布后的十年间,许多国家政府都制定了社区卫生工作者(CHW)国家方案,以此作为回应,但这些方案的评估结果往往显示效果不佳。随着许多 CHW 方案应对艾滋病毒/艾滋病大流行,国际上对 CHW 的兴趣又重新燃起,因此需要仔细审查它们在应对其他疾病方面的作用,以便吸取经验教训,将其应用于新的角色。在非洲五岁以下儿童死亡的原因中,有一半以上是疟疾、腹泻和肺炎造成的——通过 CHW 提供廉价有效的干预措施,可以解决这个问题。然而,迄今为止,在非洲,关于 CHW 方案对儿童死亡率影响的随机对照试验证据非常少。此前,关于非随机对照研究的证据尚未进行系统审查。
我们在已发表和未发表的研究数据库中搜索了 RCT 和非随机对照研究,这些研究评估了 1987 年至 2007 年期间撒哈拉以南非洲地区的 CHW 方案,这些方案提供了治疗性治疗,无论是否有预防成分,用于治疗疟疾、腹泻或肺炎,评估了这些方案对 6 岁以下儿童发病率或死亡率的影响。试图对与这些影响相关的干预和背景因素进行描述性分析。
本综述共确定了 7 项评估 CHW 的研究,评估了一系列干预措施。关于这些 CHW 方案的方案、背景或进程结果的有限描述性数据。在国家方案中,杀虫剂处理过的蚊帐和抗疟化学预防措施的提供,除了治疗干预措施外,还使 CHW 实现了分别为 63%和 36%的死亡率大幅降低。
如果在大规模实施,CHW 方案有可能在撒哈拉以南非洲地区实现儿童生存的重大改善。迫切需要大规模严格的研究,包括 RCT,为决策者提供更多关于 CHW 提供这些干预措施的效果的证据。