Reich Betzalel, Zalut Todd, Weiner Scott G
Tufts University School of Medicine, Boston, MA, USA.
Int J Emerg Med. 2011 Oct 29;4:68. doi: 10.1186/1865-1380-4-68.
Abdominal computed tomography scan (CT) is the preferred radiographic study for the diagnosis of appendicitis in the United States, while radiologist-operated ultrasound (US) is often used in Israel. This comparative international study evaluates the performance of CT vs. US in the evaluation of acute appendicitis.
A retrospective chart analysis was conducted at two tertiary care teaching hospitals, one in each country. Adult patients (age 18-99) with an Emergency Department (ED) working diagnosis of appendicitis between 1 January 2005 and 31 December 2006 were reviewed. Included patients had at least one imaging study, went to the OR, and had documented surgical pathology results.
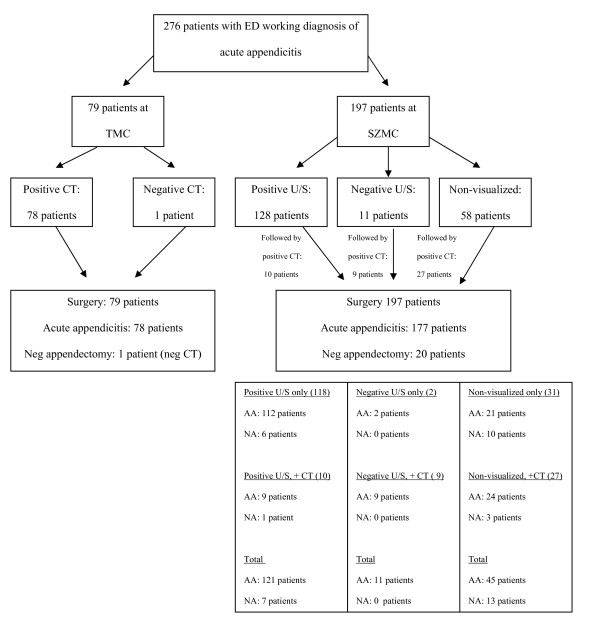
Of 136 patients in the United States with the ED diagnosis of appendicitis, 79 met inclusion criteria for the CT cohort. Based on pathology, CT had a sensitivity of 100% (95% CI 95.4-100%). The negative appendectomy rate in patients with positive CT was 0%. Total median ED length of stay was 533 min [IQR (450-632)] and median time from CT order to completion was 184 min [IQR (147-228)]. Of 520 patients in Israel, 197 were included in the US cohort. Based on final pathology, US had a sensitivity of 68.4% (95% CI 61.2-74.8%). The negative appendectomy rate in patients with positive US was 5.5%. The median ED length of stay for these patients was 387 min [IQR (259-571.5)]. Of the patients, 23.4% had subsequent CT scans. Median time from US order to completion was 20 min [IQR (7-49)]. Both time values were p < 0.001 when compared with CT. We furthermore calculate that a "first pass" approach of using US first, and then performing a confirmatory CT scan in patients with negative US, would have saved an average of 88.0 minutes per patient in the United States and avoided CT in 65% of patients.
Radiologist-operated US had inferior sensitivity and positive predictive value when compared with CT, though was significantly faster to perform, and avoided radiation and contrast in a majority of patients. A "first-pass" approach using US first and then CT if US is not diagnostic may be desirable in some institutions.
在美国,腹部计算机断层扫描(CT)是诊断阑尾炎首选的影像学检查,而在以色列,放射科医生操作的超声检查(US)则经常被使用。这项国际对比研究评估了CT与US在急性阑尾炎评估中的表现。
在两个国家的各一家三级医疗教学医院进行了回顾性病历分析。对2005年1月1日至2006年12月31日期间急诊科初步诊断为阑尾炎的成年患者(年龄18 - 99岁)进行了评估。纳入的患者至少进行了一项影像学检查,接受了手术治疗,并记录了手术病理结果。
在美国,136例急诊科诊断为阑尾炎的患者中,79例符合CT队列的纳入标准。基于病理结果,CT的敏感性为100%(95%置信区间95.4 - 100%)。CT检查结果为阳性的患者中阴性阑尾切除术的发生率为0%。急诊科总中位住院时间为533分钟[四分位间距(IQR)(450 - 632)],从开具CT检查单到完成检查的中位时间为184分钟[IQR(147 - 228)]。在以色列的520例患者中,197例被纳入超声队列。根据最终病理结果,超声的敏感性为68.4%(95%置信区间61.2 - 74.8%)。超声检查结果为阳性的患者中阴性阑尾切除术的发生率为5.5%。这些患者在急诊科的中位住院时间为387分钟[IQR(259 - 571.5)]。其中23.4%的患者随后进行了CT扫描。从开具超声检查单到完成检查的中位时间为20分钟[IQR(7 - 49)]。与CT相比,这两个时间值的p均<0.001。我们进一步计算得出,在美国采用先进行超声检查,然后对超声检查结果为阴性的患者进行CT检查进行确认的“一次通过”方法,平均每位患者可节省88.0分钟,并可使65%的患者避免接受CT检查。
与CT相比,放射科医生操作的超声检查敏感性和阳性预测值较低,不过检查速度明显更快,且在大多数患者中可避免辐射和造影剂使用。在某些机构可能适合采用先进行超声检查,若超声检查不能明确诊断则再进行CT检查的“一次通过”方法。