Department of Pathology, Johns Hopkins Medical Institutions, Baltimore, MD, USA.
Mod Pathol. 2012 Mar;25(3):378-87. doi: 10.1038/modpathol.2011.171. Epub 2011 Nov 4.
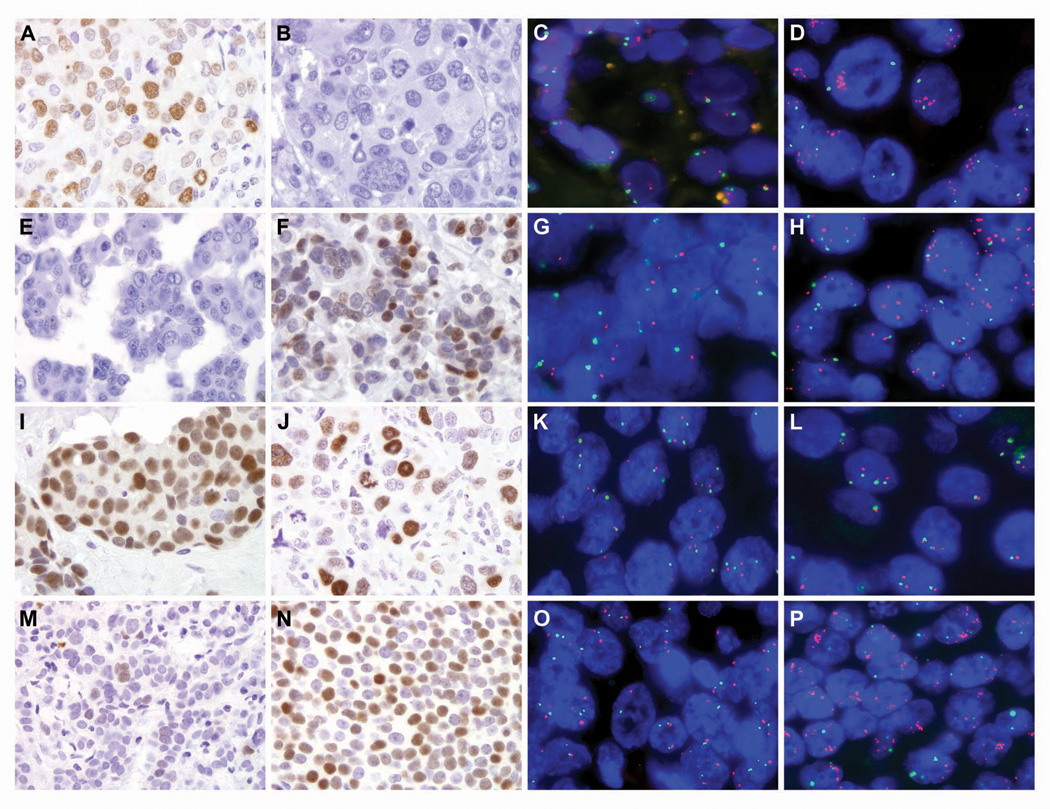
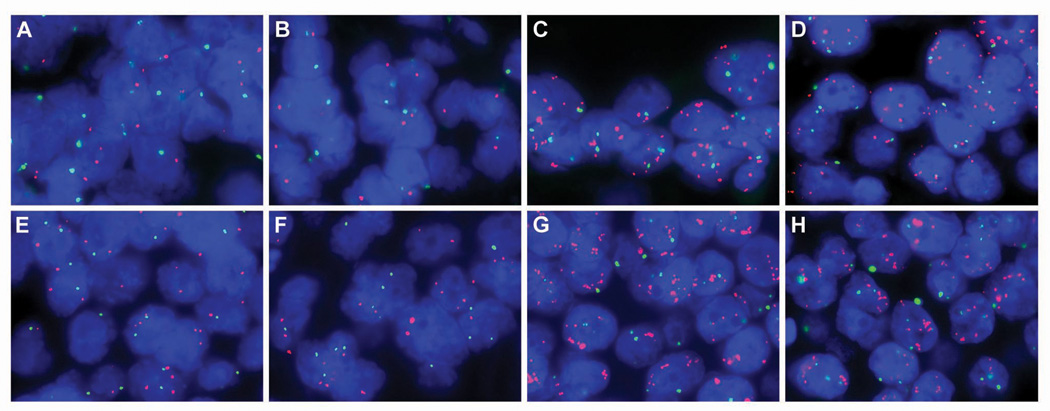
In breast cancer, amplification of MYC is consistently observed in aggressive forms of disease and correlates with poor prognosis and distant metastases. However, to date, a systematic analysis of MYC amplification in metastatic breast cancers has not been reported. Specifically, whether the MYC amplification status may change in metastases in comparison to the corresponding primary breast tumor, and potential variability among different metastases within the same patient have also not been assessed. We generated single patient tissue microarrays consisting of both primary breast carcinomas and multiple matched systemic metastases from 15 patients through our previously described rapid autopsy program. In total, the 15 tissue microarrays contained 145 primary tumor spots and 778 spots derived from 180 different metastases. In addition, two separate tissue microarrays were constructed composed of 10 matched primary breast cancers and corresponding solitary metastases sampled not at autopsy but rather in routine surgical resections. These two tissue microarrays totaled 50 primary tumor spots and 86 metastatic tumor spots. For each case, hormone receptor status, HER2/neu, EGFR and CK5/6 expression were assessed, and the cases were characterized as luminal, basal-like or HER2 based on published criteria. Both fluorescence in situ hybridization and immunohistochemistry for MYC was performed on all cases. Of the 25 cases, 24 were evaluable. While 4 of 24 primary tumors (16%) demonstrated MYC amplification, an additional 6 (25% of total evaluable cases) acquired MYC amplification in their systemic metastases. Of note, there was remarkably little heterogeneity in MYC copy number among different metastases from the same patient. MYC immunoreactivity was increased in metastases relative to matched primaries in the surgical cohort, although there was no perfect correlation with MYC amplification. In conclusion, amplification of MYC is a frequent event in breast cancer, but occurs more frequently as a diffuse, acquired event in metastatic disease than in the corresponding primary. These observations underscore the importance of MYC in breast cancer progression/metastasis, as well as its relevance as a potential therapeutic target in otherwise incurable metastatic disease.
在乳腺癌中,MYC 的扩增在侵袭性疾病中始终存在,并与不良预后和远处转移相关。然而,迄今为止,尚未有系统分析转移性乳腺癌中 MYC 扩增的报道。具体而言,与相应的原发性乳腺癌相比,转移灶中 MYC 扩增状态是否会发生变化,以及同一患者的不同转移灶之间是否存在潜在的变异性,这些都尚未得到评估。我们通过之前描述的快速尸检计划,从 15 名患者中生成了包含原发性乳腺癌和多个匹配系统性转移灶的单个患者组织微阵列。总的来说,这 15 个组织微阵列包含 145 个原发性肿瘤点和 778 个源自 180 个不同转移灶的肿瘤点。此外,还构建了两个由 10 个匹配的原发性乳腺癌和相应的非尸检但在常规手术切除中取样的单一转移灶组成的单独组织微阵列。这两个组织微阵列总计包含 50 个原发性肿瘤点和 86 个转移性肿瘤点。对于每个病例,都评估了激素受体状态、HER2/neu、EGFR 和 CK5/6 的表达,并根据已发表的标准将病例特征化为 luminal、basal-like 或 HER2。对所有病例均进行了荧光原位杂交和 MYC 的免疫组织化学检测。在 25 个病例中,有 24 个可评估。在 24 个原发性肿瘤中,有 4 个(16%)显示 MYC 扩增,而另外 6 个(总可评估病例的 25%)在其系统性转移灶中获得了 MYC 扩增。值得注意的是,来自同一患者的不同转移灶之间的 MYC 拷贝数几乎没有异质性。在手术队列中,与匹配的原发性肿瘤相比,转移灶中的 MYC 免疫反应性增加,尽管与 MYC 扩增没有完全相关性。总之,MYC 扩增在乳腺癌中是一个常见事件,但在转移性疾病中,与相应的原发性肿瘤相比,它更常作为弥漫性获得性事件发生。这些观察结果强调了 MYC 在乳腺癌进展/转移中的重要性,以及作为 otherwise incurable 转移性疾病潜在治疗靶点的相关性。