Sridhar K, Sridhar R, Venkatprasanna G
Department of Neurosurgery, Fortis Malar Hospital, Chennai, India.
J Pediatr Neurosci. 2011 Oct;6(Suppl 1):S72-7. doi: 10.4103/1817-1745.85714.
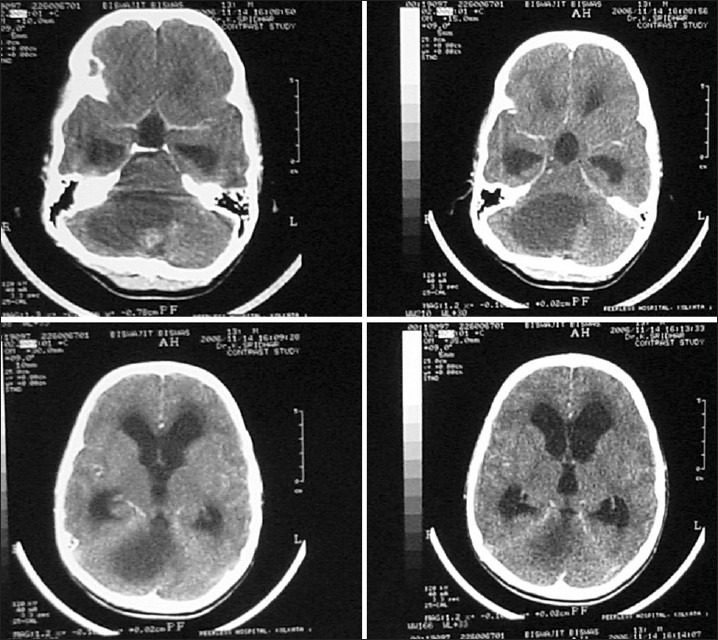
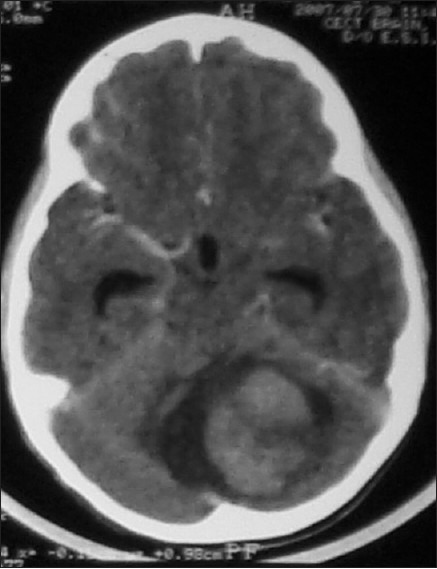
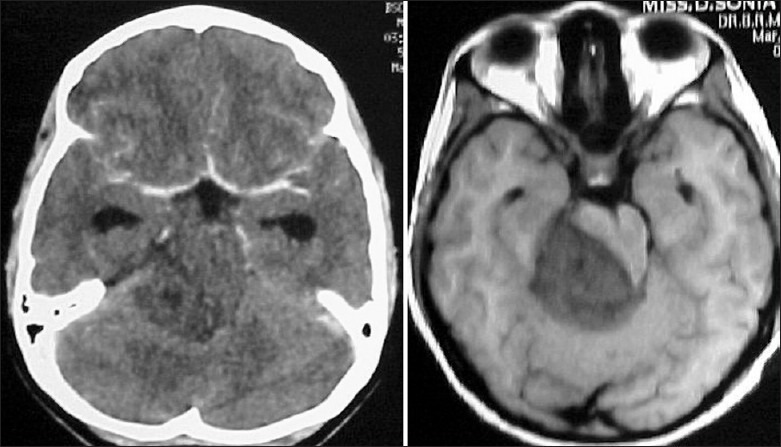
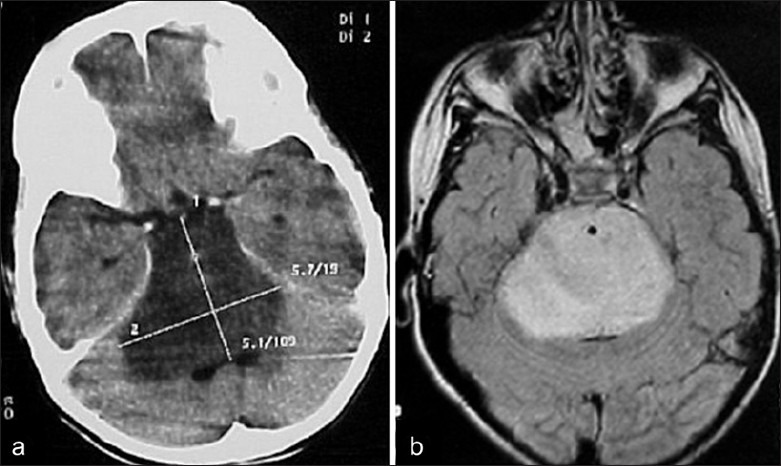
Brain tumours form the most common type of solid tumour in children and more that 50% of these are infratentorial. Cerebellar astrocytomas and brain stem gliomas are the commonest posterior fossa glial tumours in children. Cerebellar astrocytomas represent up to 10% of all primary brain tumours and up to 25% of posterior fossa tumors in children, with Low grade gliomas forming the commonest of the cerebellar gliomas. They commonly present with symptoms and signs of raised intracranial pressure due to obstructive hydrocephalus. Radiologically they may be solid or cystic with or without a mural nodule. Surgical excision is the mainstay of treatment and forms the most consistent factor influencing progression free and long term survival. While majority of the tumours are pilocytic astrocytomas, they may also be fibrillary astrocytomas or even high grade tumours. Tumour histology does not appear to be an independent factor in the prognosis of these children, and therefore no palliative treatment after surgery is advocated. Brain stem gliomas account for approximately 10% of all pediatric brain tumours. Cranial nerve signs, ataxia and cerebellar signs with or without symptoms and signs of raised intracranial pressure are classically described symptoms and signs. Radiographic findings and clinical correlates can be used to categorize brain stem tumours into four types: diffuse, focal, exophytic and cervicomedullary. Histologically most brain stem gliomas are fibrillary astrocytomas. Diffuse brain stem gliomas are the most commonly seen tumour in the brain stem. These lesions are malignant high grade fibrillary astrocytomas. Focal tumours of the brain stem are demarcated lesions generally less than 2 cms in size, without associated edema. Most commonly seen in the midbrain or medulla, they form a heterogeneous pathological group, showing indolent growth except when the lesion is a PNET. Dorsally exophytic tumours lie in the fourth ventricle, while cervicomedullary lesions are similar to spinal intramedullary tumours. Expanding lesions are the only lesions amenable for excision while infiltrative and ventral lesions are not.
脑肿瘤是儿童最常见的实体瘤类型,其中超过50%为幕下肿瘤。小脑星形细胞瘤和脑干胶质瘤是儿童最常见的后颅窝胶质肿瘤。小脑星形细胞瘤占所有原发性脑肿瘤的10%,占儿童后颅窝肿瘤的25%,低级别胶质瘤是最常见的小脑胶质瘤类型。它们通常因梗阻性脑积水而出现颅内压升高的症状和体征。影像学上,它们可以是实性或囊性,有或没有壁结节。手术切除是主要的治疗方法,也是影响无进展生存期和长期生存的最一致因素。虽然大多数肿瘤是毛细胞型星形细胞瘤,但也可能是纤维型星形细胞瘤甚至高级别肿瘤。肿瘤组织学似乎不是这些儿童预后的独立因素,因此不主张术后进行姑息治疗。脑干胶质瘤约占所有儿童脑肿瘤的10%。经典描述的症状和体征包括脑神经体征、共济失调和小脑体征,有或没有颅内压升高的症状和体征。影像学表现和临床关联可用于将脑干肿瘤分为四种类型:弥漫性、局灶性、外生性和颈髓型。组织学上,大多数脑干胶质瘤是纤维型星形细胞瘤。弥漫性脑干胶质瘤是脑干中最常见的肿瘤。这些病变是恶性高级别纤维型星形细胞瘤。脑干局灶性肿瘤是边界清晰的病变,一般大小小于2厘米,无相关水肿。最常见于中脑或延髓,它们形成一个异质性病理组,生长缓慢,除非病变是原始神经外胚层肿瘤(PNET)。背侧外生性肿瘤位于第四脑室,而颈髓病变类似于脊髓髓内肿瘤。扩展性病变是唯一适合切除的病变,而浸润性和腹侧病变则不适合。