Critical Care Unit, Hospital Israelita Albert Einstein, São Paulo, Brazil.
PLoS One. 2011;6(11):e26790. doi: 10.1371/journal.pone.0026790. Epub 2011 Nov 3.
The Surviving Sepsis Campaign (SSC) guidelines for the management of severe sepsis (SS) and septic shock (SSh) have been recommended to reduce morbidity and mortality.
A quasi-experimental study was conducted in a medical-surgical ICU. Multiple interventions to optimize SS and SSh shock patients' clinical outcomes were performed by applying sepsis bundles (6- and 24-hour) in May 2006. We compared bundle compliance and patient outcomes before (July 2005-April 2006) and after (May 2006-December 2009) implementation of the interventions.
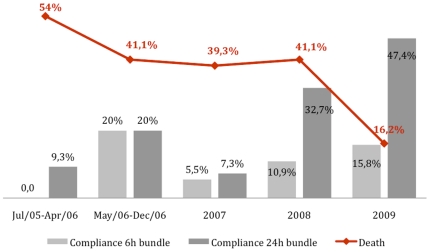
A total of 564 SS and SSh patients were identified. Prior to the intervention, compliance with the 6 hour-sepsis resuscitation bundle was only 6%. After the intervention, compliance was as follows: 8.2% from May to December 2006, 9.3% in 2007, 21.1% in 2008 and 13.7% in 2009. For the 24 hour-management bundle, baseline compliance was 15.0%. After the intervention, compliance was 15.1% from May to December 2006, 21.4% in 2007, 27.8% in 2008 and 44.4% in 2009. The in-hospital mortality was 54.0% from July 2005 to April 2006, 41.1% from May to December 2006, 39.3% in 2007, 41.4% in 2008 and 16.2% in 2009.
These results suggest reducing SS and SSh patient mortality is a complex process that involves multiple performance measures and interventions.
为了降低发病率和死亡率,《拯救脓毒症运动(SSC)严重脓毒症(SS)和脓毒性休克(SSh)管理指南》被推荐用于临床。
这是一项在外科重症监护病房(ICU)进行的准实验研究。通过 2006 年 5 月应用脓毒症包(6 小时和 24 小时)对 SS 和 SSh 休克患者进行了多项干预,以优化其临床结局。我们比较了干预前后(2005 年 7 月-2006 年 4 月和 2006 年 5 月-2009 年 12 月)包裹依从性和患者结局。
共纳入 564 例 SS 和 SSh 患者。在干预之前,6 小时脓毒症复苏包的依从性仅为 6%。干预后,依从性如下:2006 年 5 月至 12 月为 8.2%,2007 年为 9.3%,2008 年为 21.1%,2009 年为 13.7%。对于 24 小时管理包,基线依从性为 15.0%。干预后,2006 年 5 月至 12 月为 15.1%,2007 年为 21.4%,2008 年为 27.8%,2009 年为 44.4%。2005 年 7 月至 2006 年 4 月住院死亡率为 54.0%,2006 年 5 月至 12 月为 41.1%,2007 年为 39.3%,2008 年为 41.4%,2009 年为 16.2%。
这些结果表明,降低 SS 和 SSh 患者的死亡率是一个复杂的过程,需要多项绩效措施和干预措施。