Leijon Matti, Arvidsson Daniel, Nilsen Per, Stark Ekman Diana, Carlfjord Siw, Andersson Agneta, Johansson Anne Lie, Bendtsen Preben
Center for Primary Health Care Research, Lund University/Region Skåne, Malmö, Sweden.
J Med Internet Res. 2011 Nov 22;13(4):e99. doi: 10.2196/jmir.1745.
Interactive behavior change technology (eg, computer programs, Internet websites, and mobile phones) may facilitate the implementation of lifestyle behavior interventions in routine primary health care. Effective, fully automated solutions not involving primary health care staff may offer low-cost support for behavior change.
We explored the effectiveness of an electronic screening and brief intervention (e-SBI) deployed through a stand-alone information kiosk for promoting physical activity among sedentary patients in routine primary health care. We further tested whether its effectiveness differed between patients performing the e-SBI on their own initiative and those referred to it by primary health care staff.
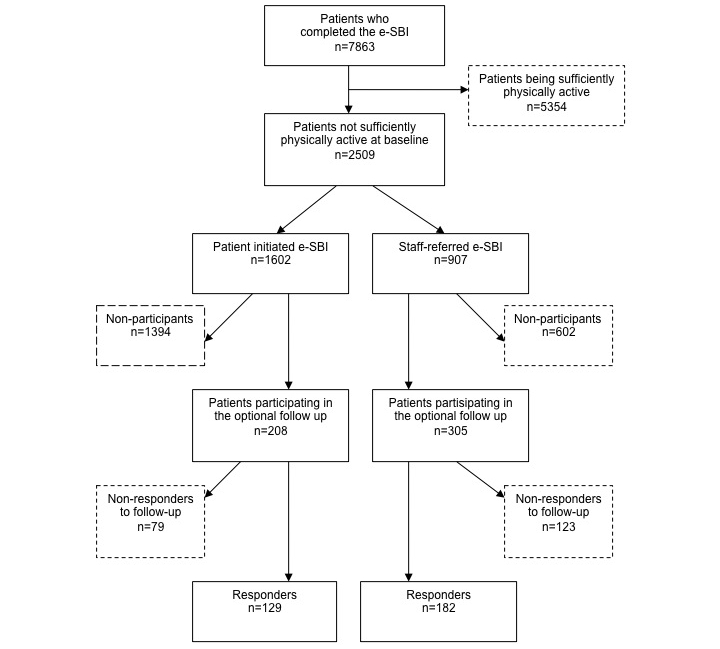
The e-SBI screens for the physical activity level, motivation to change, attitudes toward performing the test, and physical characteristics and provides tailored feedback supporting behavior change. A total of 7863 patients performed the e-SBI from 2007 through 2009 in routine primary health care in Östergötland County, Sweden. Of these, 2509 were considered not sufficiently physically active, and 311 of these 2509 patients agreed to participate in an optional 3-month follow-up. These 311 patients were included in the analysis and were further divided into two groups based on whether the e-SBI was performed on the patient´s own initiative (informed by posters in the waiting room) or if the patient was referred to it by staff. A physical activity score representing the number of days being physically active was compared between baseline e-SBI and the 3-month follow-up. Based on physical activity recommendations, a score of 5 was considered the cutoff for being sufficiently physically active.
In all, 137 of 311 patients (44%) were sufficiently physically active at the 3-month follow-up. The proportion becoming sufficiently physically active was 16/55 (29%), 40/101 (40%), and 81/155 (52%) for patients with a physical activity score at baseline of 0, 1 to 2, and 3 to 4, respectively. The patient-initiated group and staff-referred group had similar mean physical activity scores at baseline (2.1, 95% confidence interval [CI] 1.8-2.3, versus 2.3, 95% CI 2.1-2.5) and at follow-up, (4.1, 95% CI 3.4-4.7, vs 4.2, 95% CI 3.7-4.8).
Among the sedentary patients in primary health care who participated in the follow-up, the e-SBI appeared effective at promoting short-term improvement of physical activity for about half of them. The results were similar when the e-SBI was patient-initiated or staff-referred. The e-SBI may be a low-cost complement to lifestyle behavior interventions in routine primary health care and could work as a stand-alone technique not requiring the involvment of primary health care staff.

交互式行为改变技术(如计算机程序、互联网网站和手机)可能有助于在常规初级卫生保健中实施生活方式行为干预。不涉及初级卫生保健人员的有效、全自动解决方案可能为行为改变提供低成本支持。
我们探讨了通过独立信息亭部署的电子筛查与简短干预(e-SBI)在常规初级卫生保健中促进久坐患者身体活动的有效性。我们还测试了主动进行e-SBI的患者与由初级卫生保健人员转诊的患者之间其有效性是否存在差异。
e-SBI会筛查身体活动水平、改变的动机、对进行测试的态度以及身体特征,并提供支持行为改变的个性化反馈。2007年至2009年期间,瑞典东约特兰郡共有7863名患者在常规初级卫生保健中进行了e-SBI。其中,2509人被认为身体活动不足,这2509名患者中有311人同意参加为期3个月的可选随访。这311名患者被纳入分析,并根据e-SBI是患者主动进行(通过候诊室的海报得知)还是由工作人员转诊进一步分为两组。比较了基线e-SBI和3个月随访时代表身体活动天数的身体活动得分。根据身体活动建议,5分被视为身体活动充足的临界值。
总体而言,311名患者中有137名(44%)在3个月随访时身体活动充足。基线身体活动得分为0、1至2、3至4的患者,身体活动变得充足的比例分别为16/55(29%)、40/101(40%)和81/155(52%)。患者主动组和工作人员转诊组在基线时(分别为2.1,95%置信区间[CI]1.8 - 2.3,与2.3,95%CI 2.1 - 2.5)和随访时(分别为4.1,95%CI 3.4 - 4.7,与4.2,95%CI 3.7 - 4.8)的平均身体活动得分相似。
在参与随访的初级卫生保健久坐患者中,e-SBI似乎对约一半患者有效促进了身体活动的短期改善。无论是患者主动进行还是工作人员转诊,e-SBI的结果相似。e-SBI可能是常规初级卫生保健中生活方式行为干预的低成本补充,并且可以作为一种无需初级卫生保健人员参与的独立技术发挥作用。