Pefura Yone Eric Walter, Kengne André Pascal, Kuaban Christopher
Department of Internal Medicine and Specialties, Faculty of Medicine and Biomedical Sciences, The University of Yaounde I, Yaounde, Cameroon.
BMJ Open. 2011 Nov 24;1(2):e000289. doi: 10.1136/bmjopen-2011-000289. Print 2011.
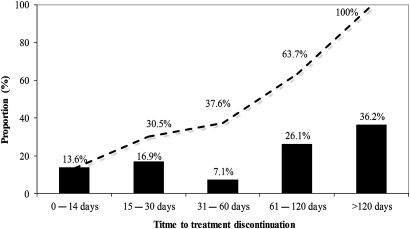
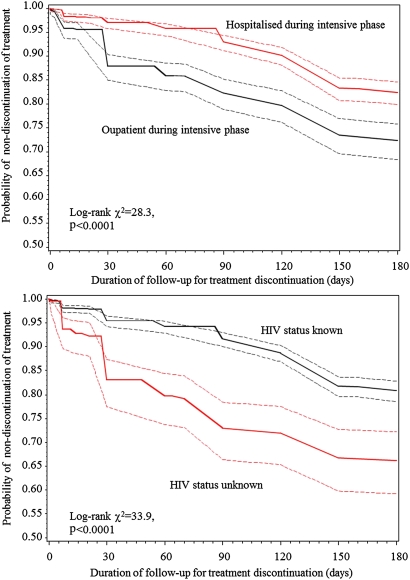
Objectives High rates of antituberculosis treatment discontinuation have been reported in some areas of Africa. The aim of this study was to determine the rate, time to and determinants of antituberculosis treatment default in Yaounde. Design This was a retrospective cohort study based on hospital registers. Tuberculosis treatment default or antituberculosis treatment discontinuation was defined as any interruption of treatment for at least 2 months following treatment initiation. Sociodemographic and clinical predictors of treatment discontinuation were investigated with the use of Cox regressions models. Setting This study was carried out in the tuberculosis diagnosis and treatment centre at Yaounde Jamot Hospital, which serves as a referral centre for tuberculosis and respiratory diseases for the capital city of Cameroon (Yaounde) and surrounding areas. Participants All (1688) patients started on antituberculosis treatment at the centre between January and December 2009 were enrolled. Outcome measures were antituberculosis treatment default and time to treatment default. Results Of the 1688 included patients, 337 (20%) defaulted from treatment, 86 (5.1%) died, treatment failed in 6 (0.4%) and 104 (6.2%) were transferred. Therefore, treatment was successfully completed in 1154 (68.4%) patients. Median duration to treatment discontinuation was 90 days (IQR 30-150), and 62% of treatment discontinuation occurred during the continuation phase. Hospitalisation during the intensive phase (adjusted HR 0.69; 95% CI 0.54 to 0.89) and non-consenting for HIV screening (1.65; 1.24 to 2.21) were the main determinants of defaulting from treatment in multivariable analysis. Conclusions The default incidence rate is relatively high in this centre and treatment discontinuation occurs frequently during the continuation phase of treatment. Action is needed to improve adherence to treatment when received on an ambulatory basis, to clarify the association between HIV testing and antituberculosis treatment default, and to identify other potential determinants of treatment discontinuation in this setting.
目标 在非洲一些地区,抗结核治疗中断率较高。本研究旨在确定雅温得市抗结核治疗中断的发生率、发生时间及决定因素。设计 这是一项基于医院登记册的回顾性队列研究。抗结核治疗中断或停止被定义为治疗开始后至少连续2个月中断治疗。使用Cox回归模型研究治疗中断的社会人口学和临床预测因素。背景 本研究在雅温得贾莫特医院的结核病诊断和治疗中心开展,该中心是喀麦隆首都雅温得市及周边地区结核病和呼吸道疾病的转诊中心。参与者 纳入了2009年1月至12月期间在该中心开始接受抗结核治疗的所有(1688名)患者。观察指标为抗结核治疗中断情况及治疗中断时间。结果 在纳入的1688名患者中,337名(20%)中断治疗,86名(5.1%)死亡,6名(0.4%)治疗失败,104名(6.2%)被转诊。因此,1154名(68.4%)患者成功完成治疗。治疗中断的中位持续时间为90天(四分位间距30 - 150天),62%的治疗中断发生在继续治疗阶段。多变量分析中,强化治疗阶段住院(调整后风险比0.69;95%置信区间0.54至0.89)和不同意进行HIV筛查(1.65;1.24至2.21)是治疗中断的主要决定因素。结论 该中心的治疗中断发生率相对较高,且治疗中断在治疗的继续阶段频繁发生。需要采取行动提高门诊治疗时的治疗依从性,阐明HIV检测与抗结核治疗中断之间的关联,并确定该环境下治疗中断的其他潜在决定因素。