Lancet. 2012 Feb 4;379(9814):432-44. doi: 10.1016/S0140-6736(11)61625-5. Epub 2011 Dec 5.
Moderate differences in efficacy between adjuvant chemotherapy regimens for breast cancer are plausible, and could affect treatment choices. We sought any such differences.
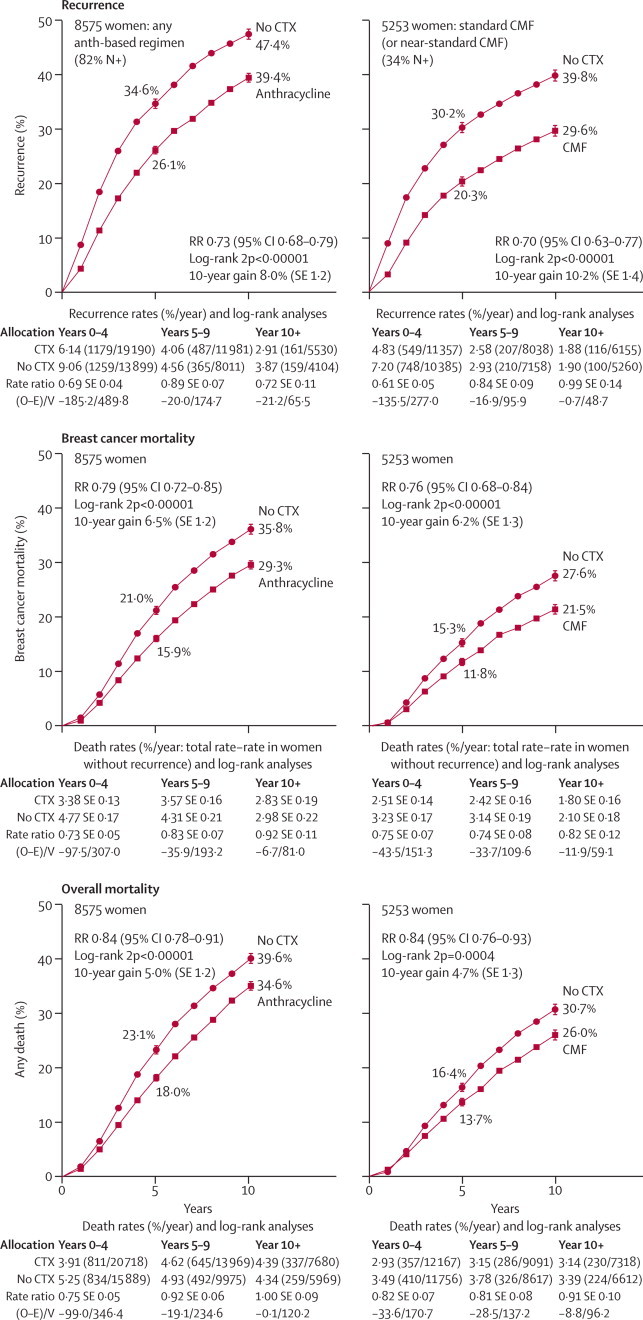
We undertook individual-patient-data meta-analyses of the randomised trials comparing: any taxane-plus-anthracycline-based regimen versus the same, or more, non-taxane chemotherapy (n=44,000); one anthracycline-based regimen versus another (n=7000) or versus cyclophosphamide, methotrexate, and fluorouracil (CMF; n=18,000); and polychemotherapy versus no chemotherapy (n=32,000). The scheduled dosages of these three drugs and of the anthracyclines doxorubicin (A) and epirubicin (E) were used to define standard CMF, standard 4AC, and CAF and CEF. Log-rank breast cancer mortality rate ratios (RRs) are reported.
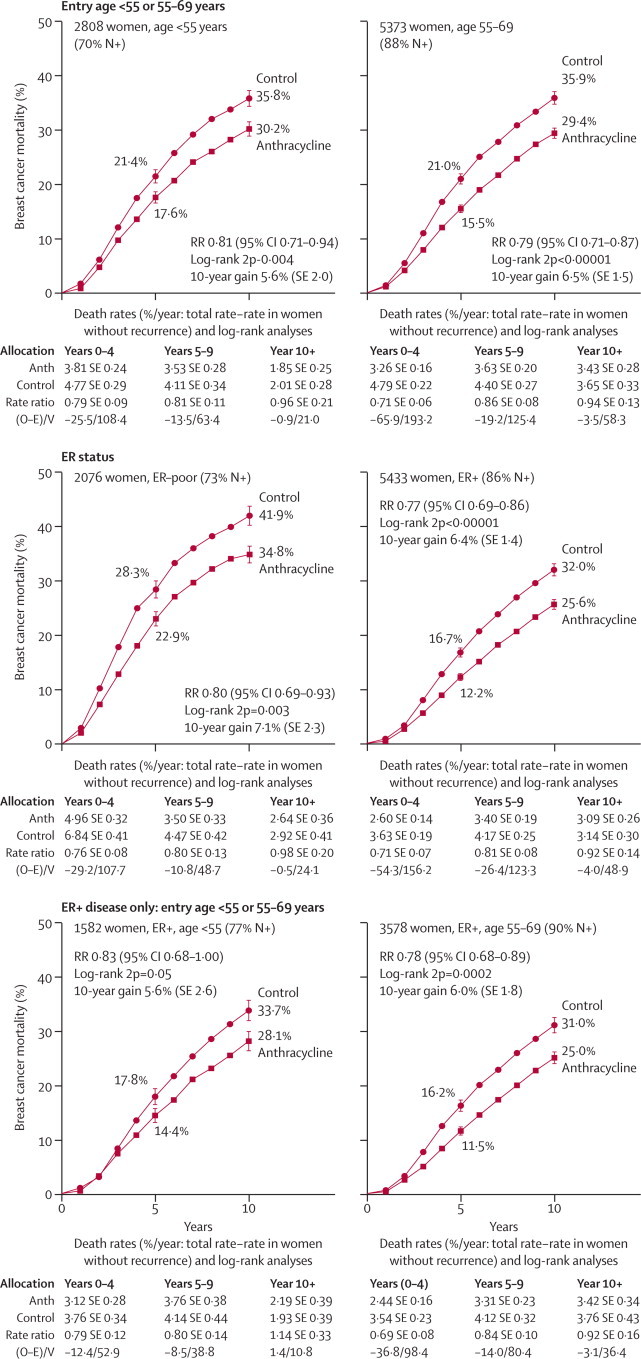
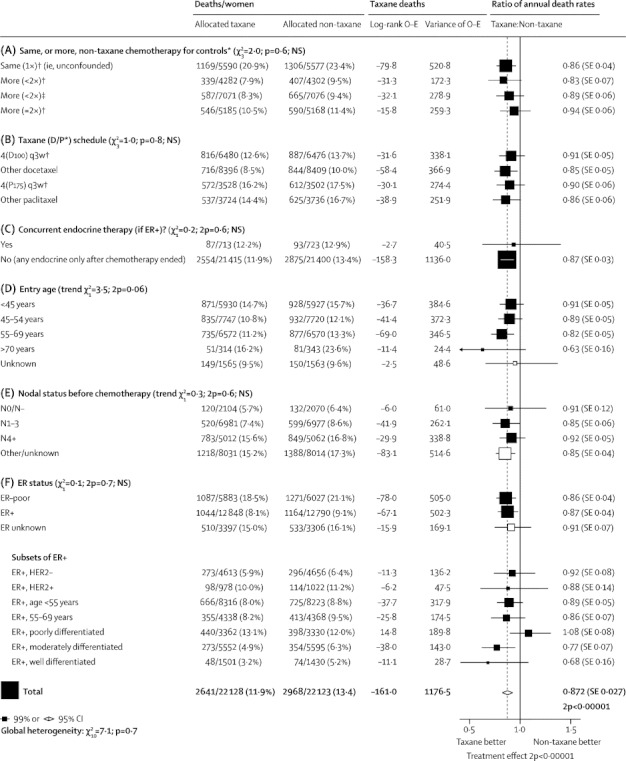
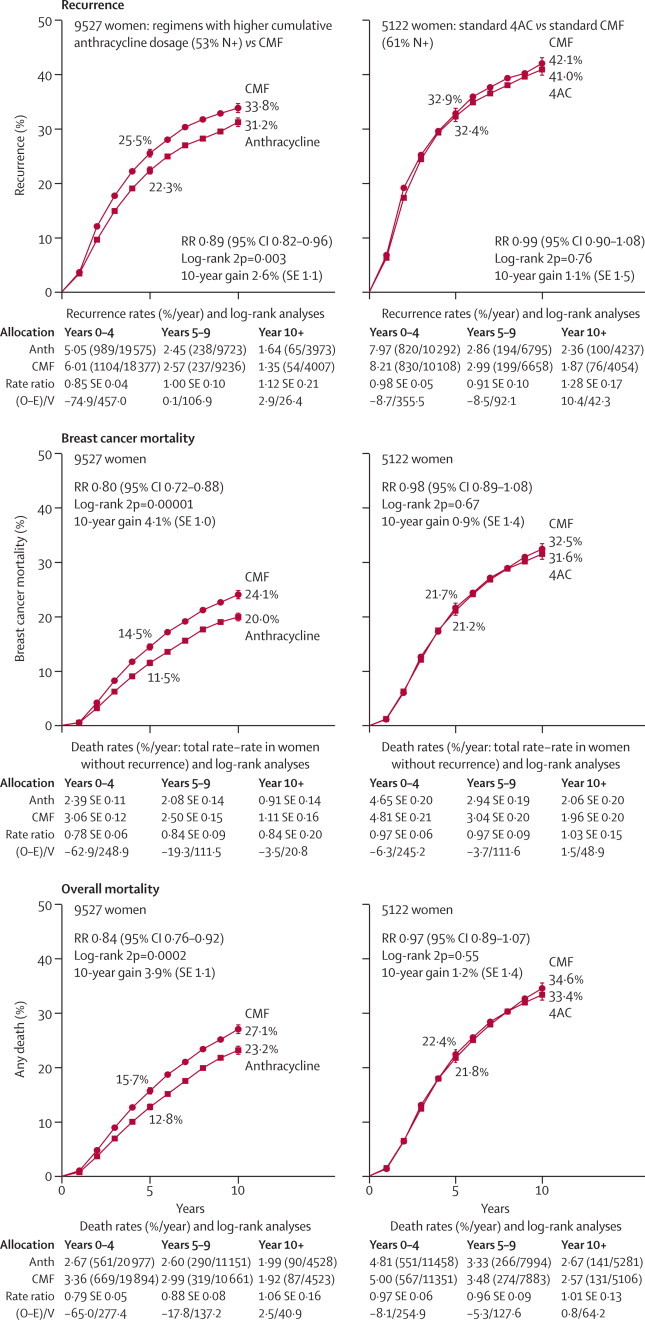
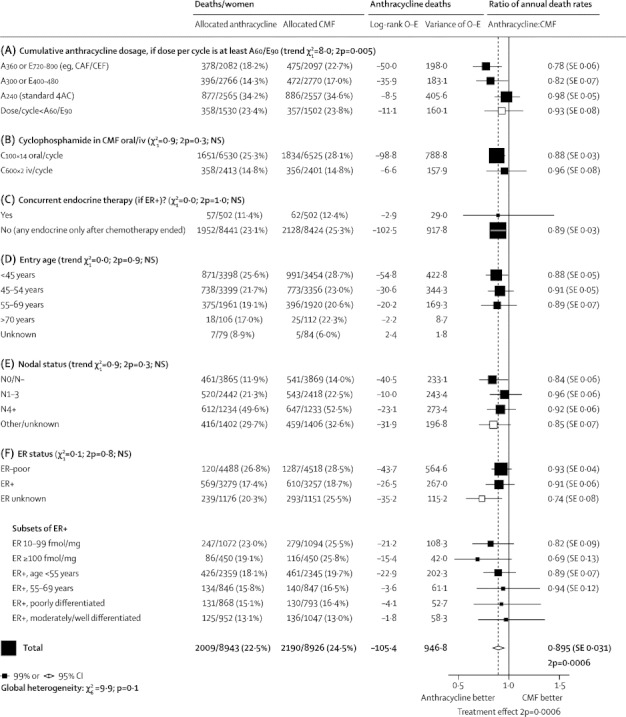
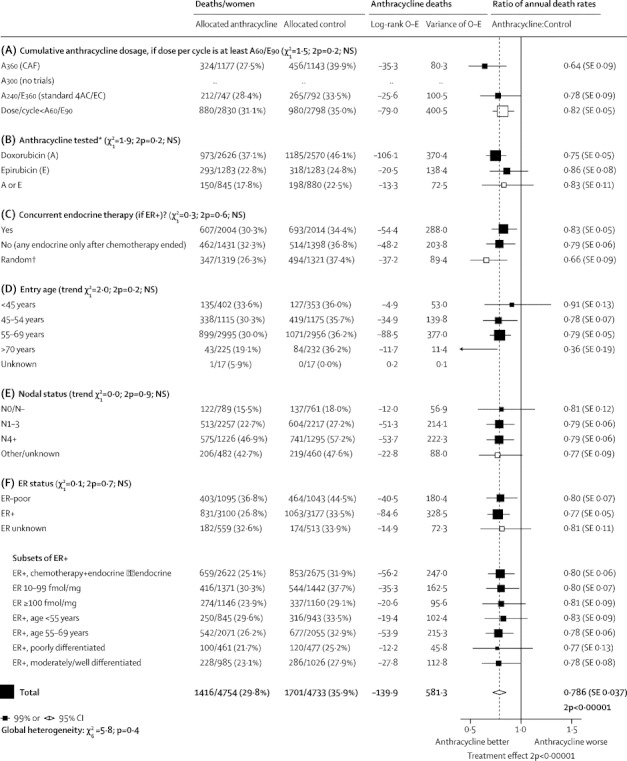
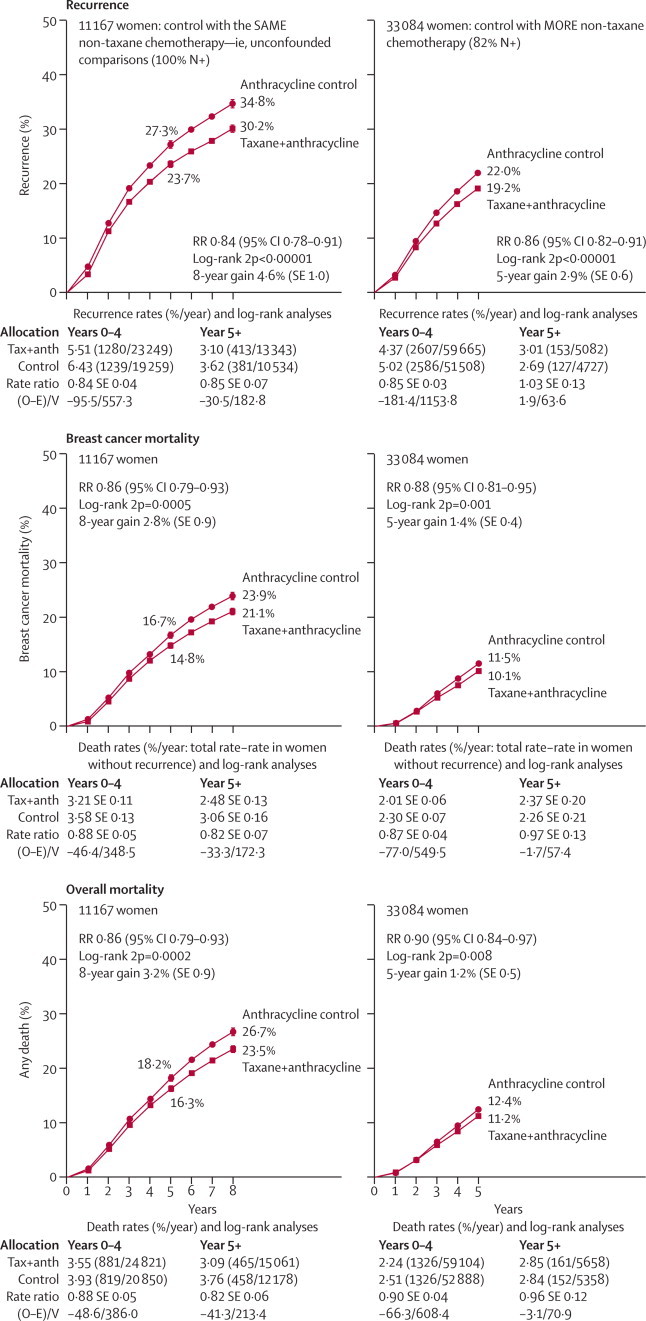
In trials adding four separate cycles of a taxane to a fixed anthracycline-based control regimen, extending treatment duration, breast cancer mortality was reduced (RR 0·86, SE 0·04, two-sided significance [2p]=0·0005). In trials with four such extra cycles of a taxane counterbalanced in controls by extra cycles of other cytotoxic drugs, roughly doubling non-taxane dosage, there was no significant difference (RR 0·94, SE 0·06, 2p=0·33). Trials with CMF-treated controls showed that standard 4AC and standard CMF were equivalent (RR 0·98, SE 0·05, 2p=0·67), but that anthracycline-based regimens with substantially higher cumulative dosage than standard 4AC (eg, CAF or CEF) were superior to standard CMF (RR 0·78, SE 0·06, 2p=0·0004). Trials versus no chemotherapy also suggested greater mortality reductions with CAF (RR 0·64, SE 0·09, 2p<0·0001) than with standard 4AC (RR 0·78, SE 0·09, 2p=0·01) or standard CMF (RR 0·76, SE 0·05, 2p<0·0001). In all meta-analyses involving taxane-based or anthracycline-based regimens, proportional risk reductions were little affected by age, nodal status, tumour diameter or differentiation (moderate or poor; few were well differentiated), oestrogen receptor status, or tamoxifen use. Hence, largely independently of age (up to at least 70 years) or the tumour characteristics currently available to us for the patients selected to be in these trials, some taxane-plus-anthracycline-based or higher-cumulative-dosage anthracycline-based regimens (not requiring stem cells) reduced breast cancer mortality by, on average, about one-third. 10-year overall mortality differences paralleled breast cancer mortality differences, despite taxane, anthracycline, and other toxicities.
10-year gains from a one-third breast cancer mortality reduction depend on absolute risks without chemotherapy (which, for oestrogen-receptor-positive disease, are the risks remaining with appropriate endocrine therapy). Low absolute risk implies low absolute benefit, but information was lacking about tumour gene expression markers or quantitative immunohistochemistry that might help to predict risk, chemosensitivity, or both.
Cancer Research UK; British Heart Foundation; UK Medical Research Council.
乳腺癌辅助化疗方案之间的疗效差异可能是合理的,并且可能会影响治疗选择。我们旨在寻找这些差异。
我们对比较:任何紫杉烷加蒽环类药物方案与相同或更多非紫杉烷化疗(n=44000);一种蒽环类药物方案与另一种(n=7000)或与环磷酰胺、甲氨蝶呤和氟尿嘧啶(CMF;n=18000);以及多化疗与无化疗(n=32000)的随机试验进行了基于个体患者数据的荟萃分析。这些三种药物和蒽环类药物阿霉素(A)和表阿霉素(E)的计划剂量用于定义标准 CMF、标准 4AC 和 CAF 和 CEF。报告预定的乳腺癌死亡率比率(RR)。
在试验中,将四种单独的紫杉烷周期添加到固定的基于蒽环类药物的对照方案中,延长治疗持续时间,乳腺癌死亡率降低(RR 0.86,SE 0.04,双侧显著性[2p]=0.0005)。在具有四个额外紫杉烷周期的试验中,在对照中通过其他细胞毒性药物的额外周期平衡,大致增加非紫杉烷剂量,没有显著差异(RR 0.94,SE 0.06,2p=0.33)。使用 CMF 治疗对照的试验表明,标准 4AC 和标准 CMF 是等效的(RR 0.98,SE 0.05,2p=0.67),但与标准 4AC 相比,累积剂量更高的蒽环类药物方案(例如 CAF 或 CEF)优于标准 CMF(RR 0.78,SE 0.06,2p=0.0004)。与无化疗的试验也表明,CAF 比标准 4AC(RR 0.78,SE 0.09,2p=0.01)或标准 CMF(RR 0.76,SE 0.05,2p<0.0001)更能降低死亡率。在涉及紫杉烷或蒽环类药物方案的所有荟萃分析中,比例风险降低受年龄、淋巴结状态、肿瘤直径或分化(中或差;很少是高分化)、雌激素受体状态或他莫昔芬使用的影响较小。因此,在很大程度上独立于年龄(至少 70 岁)或我们目前为这些试验选择的患者的肿瘤特征,一些紫杉烷加蒽环类药物或更高累积剂量的蒽环类药物方案(不需要干细胞)平均降低了约三分之一的乳腺癌死亡率。10 年总死亡率差异与乳腺癌死亡率差异平行,尽管存在紫杉烷、蒽环类药物和其他毒性。
三分之一乳腺癌死亡率降低的 10 年获益取决于无化疗的绝对风险(对于雌激素受体阳性疾病,这是适当内分泌治疗后残留的风险)。低绝对风险意味着低绝对获益,但缺乏有关肿瘤基因表达标志物或定量免疫组织化学的信息,这些信息可能有助于预测风险、化疗敏感性或两者。
英国癌症研究中心;英国心脏基金会;英国医学研究理事会。