Division of Image Processing, Department of Radiology, Leiden University Medical Center, Albinusdreef 2, 2300 RC Leiden, The Netherlands.
Int J Cardiovasc Imaging. 2012 Oct;28(7):1617-25. doi: 10.1007/s10554-011-9996-x. Epub 2011 Dec 15.
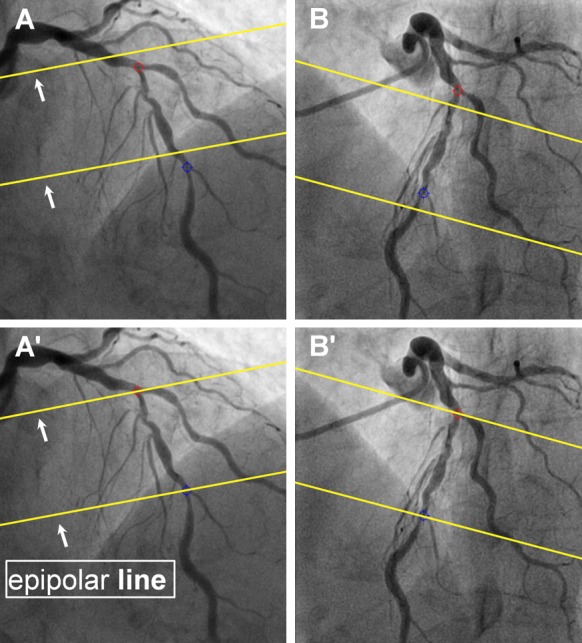
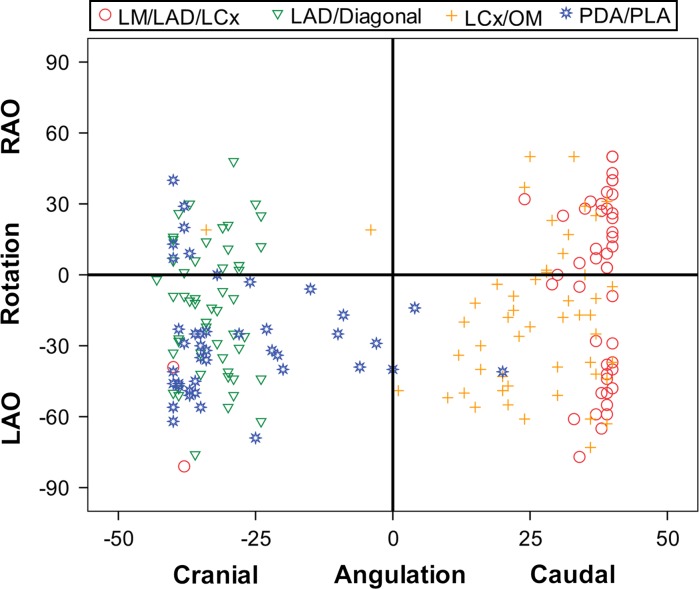
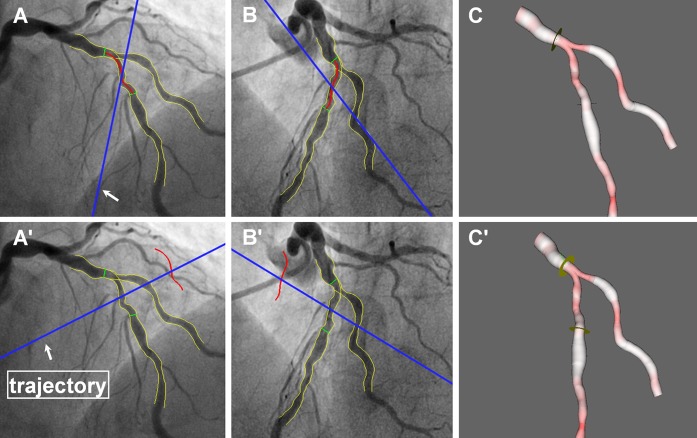
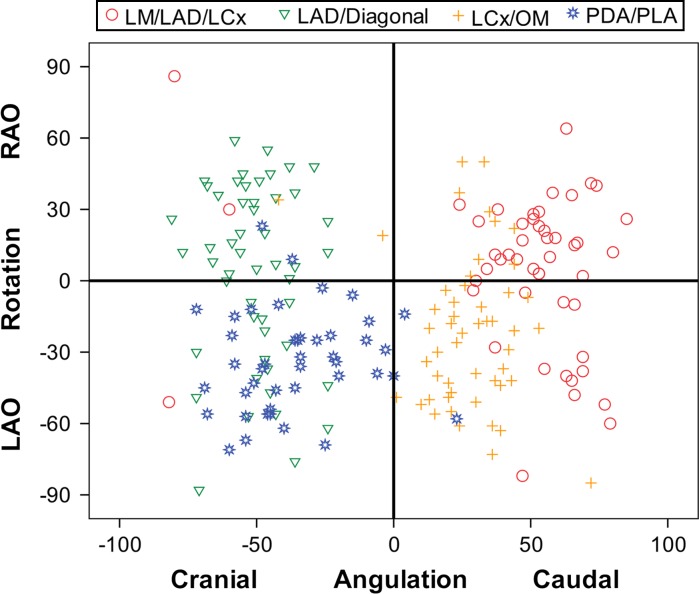
Evaluation and stenting of coronary bifurcation lesions may benefit from optimal angiographic views. The anatomy-defined bifurcation optimal viewing angle (ABOVA) is characterized by having an orthogonal view of the bifurcation, such that overlap and foreshortening at the ostium are minimized. However, due to the mechanical constraints of the X-ray systems, certain deep angles cannot be reached by the C-arm. Therefore, second best or, so-called obtainable bifurcation optimal viewing angle (OBOVA) has to be used as an alternative. This study assessed the distributions of ABOVA and OBOVA using 3D quantitative coronary angiography in a typical patient population. In addition, the bifurcation angles in four main coronary bifurcations were assessed and compared. Patients with obstructive coronary bifurcation disease were included in this multicenter registry. A novel and validated 3D QCA software package was applied to reconstruct the bifurcations and to calculate the bifurcation angles in 3D. A list of optimal viewing angle candidates including ABOVA was also automatically proposed by the software. In a next step, the operator selected the best viewing angle as OBOVA, while applying a novel overlap prediction approach to assure no overlap between the target bifurcation and other major coronary arteries. A total of 194 bifurcations from 181 patients were assessed. The ABOVA could not be reached in 56.7% of the cases; being 40 (81.6%), 40 (78.4%), 9 (17.6%), and 21 (48.8%) cases for LM/LAD/LCx, LAD/Diagonal, LCx/OM, and PDA/PLA, respectively. Both ABOVA and OBOVA distributed sparsely with large ranges of variance: LM/LAD/LCx, 5 ± 33 RAO, 47 ± 35 Caudal versus 4 ± 39 LAO, 35 ± 16 Caudal; LAD/Diagonal, 4 ± 38 RAO, 50 ± 14 Cranial versus 14 ± 28 LAO, 33 ± 5 Cranial; LCx/OM, 21 ± 32 LAO, 27 ± 17 Caudal versus 18 ± 31 LAO, 25 ± 13 Caudal; PDA/PLA, 34 ± 21 LAO, 36 ± 21 Cranial versus 28 ± 25 LAO, 29 ± 15 Cranial. LM/LAD/LCx had the smallest proximal bifurcation angle (128° ± 24°) and the largest distal bifurcation angle (80° ± 21°), as compared with LAD/Diagonal (151° ± 13º and 48° ± 16º), LCx/OM (146° ± 18º and 57° ± 16°), and PDA/PLA (145° ± 19° and 59° ± 17°). In conclusion, large variabilities in optimal viewing angles existed for all main coronary bifurcations. The anatomy-defined bifurcation optimal viewing angle could not be reached in vivo in roughly half of the cases due to the mechanical constraints of the current X-ray systems. Obtainable bifurcation optimal viewing angle should be provided as an alternative or second best. The bifurcation angles in the left main bifurcation demonstrated the largest variabilities.
评估和支架置入冠状动脉分叉病变可能受益于最佳的血管造影视图。解剖定义的分叉最佳观察角度(ABOVA)的特点是具有分叉的正交视图,使得在口部的重叠和缩短最小化。然而,由于 X 射线系统的机械限制,某些深角度不能被 C 臂到达。因此,必须使用第二好的或所谓的可获得的分叉最佳观察角度(OBOVA)作为替代。本研究使用 3D 定量冠状动脉造影术评估了典型患者人群中 ABOVA 和 OBOVA 的分布。此外,评估了四个主要冠状动脉分叉的分叉角度并进行了比较。该多中心登记册纳入了有阻塞性冠状动脉分叉病变的患者。应用一种新的和经过验证的 3D QCA 软件包来重建分叉,并在 3D 中计算分叉角度。该软件还自动列出了最佳观察角度的候选列表,包括 ABOVA。在下一步中,操作者选择最佳观察角度作为 OBOVA,同时应用一种新的重叠预测方法来确保目标分叉和其他主要冠状动脉之间没有重叠。评估了 181 名患者的 194 个分叉。在大约 56.7%的情况下无法达到 ABOVA;40 个(81.6%)、40 个(78.4%)、9 个(17.6%)和 21 个(48.8%)分别为 LM/LAD/LCx、LAD/对角支、LCx/OM 和 PDA/PLA。ABOVA 和 OBOVA 的分布都很稀疏,方差范围很大:LM/LAD/LCx,5±33 RAO,47±35尾侧与 4±39 LAO,35±16 尾侧;LAD/对角支,4±38 RAO,50±14 头侧与 14±28 LAO,33±5 头侧;LCx/OM,21±32 LAO,27±17 尾侧与 18±31 LAO,25±13 尾侧;PDA/PLA,34±21 LAO,36±21 头侧与 28±25 LAO,29±15 头侧。LM/LAD/LCx 的近侧分叉角最小(128°±24°),远侧分叉角最大(80°±21°),与 LAD/对角支(151°±13°和 48°±16°)、LCx/OM(146°±18°和 57°±16°)和 PDA/PLA(145°±19°和 59°±17°)相比。总之,所有主要冠状动脉分叉的最佳观察角度都存在很大的变异性。由于当前 X 射线系统的机械限制,ABOVA 在大约一半的病例中无法在体内达到。应提供可获得的分叉最佳观察角度作为替代或第二好的选择。左主干分叉的分叉角度表现出最大的变异性。