Division of Cardiovascular Diseases, Department of Medicine, Mayo Clinic, 200 First Street, SW, Rochester, MN 55905, USA.
Heart. 2012 Mar;98(5):389-94. doi: 10.1136/heartjnl-2011-300823. Epub 2011 Dec 22.
Disease progression in heart failure (HF) reflects derangements in neurohormonal systems, and biomarkers of these systems can help to establish the diagnosis and assess the prognosis. Serial measurements of the precursor peptides of the natriuretic and vasopressin systems (midregional proatrial natriuretic peptide (MR-proANP) and C-terminal provasopressin (copeptin), respectively) should add incremental value to risk stratification in ambulatory patients with HF.
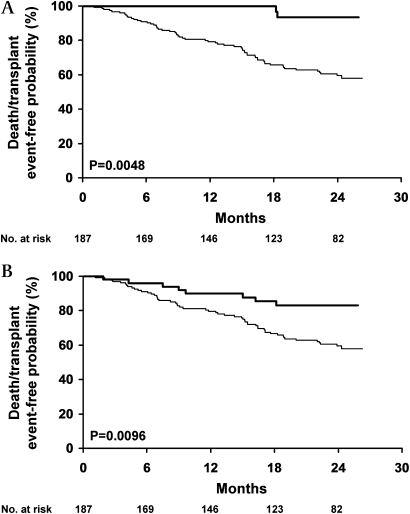
A cohort of 187 patients with class III-IV HF was prospectively enrolled, with biomarkers collected every 3 months over 2 years and analysed in relation to death/transplantation. Time-dependent analyses (dichotomous and continuous variables) showed that increases in MR-proANP (HR 7.6, 95% CI 1.85 to 31.15, p<0.01) and copeptin (HR 2.7, 95% CI 1.27 to 5.61, p=0.01) were associated with increased risk, but, in multivariate analysis adjusted for troponin T (cTnT) ≥0.01 ng/ml, only raised MR-proANP remained an independent predictor (HR 5.49, 95% CI 1.31 to 23.01, p=0.02). Combined increases in MR-proANP and copeptin (HR 9.01, 95% CI 1.24 to 65.26, p=0.03) with cTnT (HR 11.1, 95% CI 1.52 to 80.85, p=0.02), and increases ≥30% above already raised values identified the patients at greatest risk (MR-proANP: HR 10.1, 95% CI 2.34 to 43.38, p=0.002; copeptin: HR 11.5, 95% CI 2.74 to 48.08, p<0.001).
A strategy of serial monitoring of MR-proANP and, of lesser impact, copeptin, combined with cTnT, may be advantageous in detecting and managing the highest-risk outpatients with HF.
心力衰竭(HF)的疾病进展反映了神经激素系统的紊乱,这些系统的生物标志物有助于确定诊断和评估预后。利钠肽和血管加压素系统前体肽(分别为中段心房利钠肽前体(MR-proANP)和 C 末端加压素(copeptin))的连续测量应该为 HF 门诊患者的危险分层增加额外的价值。
前瞻性纳入了 187 名 III-IV 级 HF 患者,每 3 个月收集一次生物标志物,在 2 年内进行分析,并与死亡/移植相关。时间依赖性分析(二分类和连续变量)显示,MR-proANP(HR 7.6,95%CI 1.85 至 31.15,p<0.01)和 copeptin(HR 2.7,95%CI 1.27 至 5.61,p=0.01)的增加与风险增加相关,但在调整肌钙蛋白 T(cTnT)≥0.01ng/ml 的多变量分析中,只有升高的 MR-proANP 仍然是独立的预测因子(HR 5.49,95%CI 1.31 至 23.01,p=0.02)。MR-proANP 和 copeptin(HR 9.01,95%CI 1.24 至 65.26,p=0.03)与 cTnT(HR 11.1,95%CI 1.52 至 80.85,p=0.02)的联合增加,以及增加≥30%超过已经升高的值,确定了风险最大的患者(MR-proANP:HR 10.1,95%CI 2.34 至 43.38,p=0.002;copeptin:HR 11.5,95%CI 2.74 至 48.08,p<0.001)。
连续监测 MR-proANP,以及影响较小的 copeptin,与 cTnT 相结合,可能有利于检测和管理 HF 门诊患者的最高风险人群。