Barcelona Centre for International Health Research (CRESIB), Hospital Clínic Universitat de Barcelona, Barcelona, Spain.
PLoS Negl Trop Dis. 2011 Dec;5(12):e1325. doi: 10.1371/journal.pntd.0001325. Epub 2011 Dec 27.
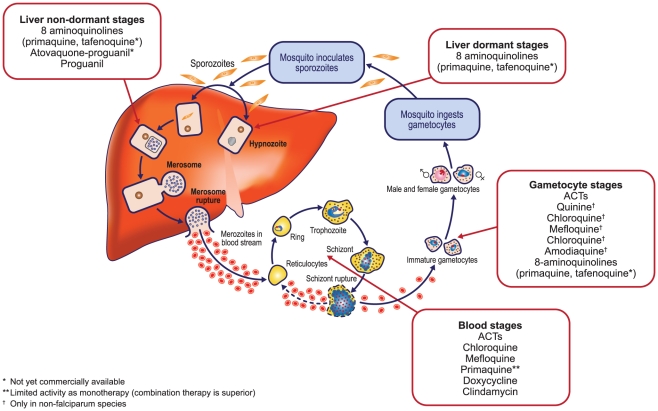
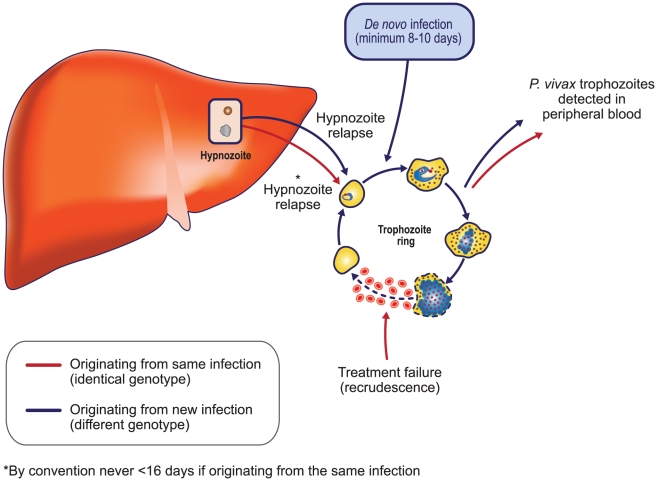
The long-standing dearth of knowledge surrounding Plasmodium vivax, the most widely distributed of the malaria species, merits urgent attention. A growing awareness of the true burden of this parasite and its potential to cause severe disease, and the identification of increasing parasite resistance in many areas of the world to chloroquine, the mainstay of vivax treatment, underscores the need to identify new and effective treatment strategies. Artemisinin-based combination therapies (ACTs) have been widely adopted as first-line treatment for P. falciparum malaria and would offer logistic benefits in areas of co-endemicity. However, while ACTs show high and similar efficacy against the blood stages of P. vivax, neither ACTs nor chloroquine are active against vivax hypnozoites and must be complemented with a full course of primaquine to eradicate dormant vivax hypnozoites and prevent relapses. Artemether-lumefantrine (AL), the most commonly deployed ACT, has shown rapid clearance of P. vivax parasitemia and fever. The relatively short half-life of lumefantrine would appear beneficial in terms of reducing risk of resistance when compared to other ACTs. However, it has a shorter capability to suppress vivax relapses or prevent de novo infections, which generally translates into comparatively lower in vivo short-term measures of efficacy (e.g., day 28 or day 42 uncorrected cure rates). Assuming that the different artemisinin derivatives have equivalent efficacy against vivax, differences between AL and other ACTs may be restricted to the duration of plasma therapeutic levels of the partner drug, a variable of limited clinical relevance, particularly in regions with low vivax transmission rates or in cases where primaquine is added to the regimen to prevent relapses. More rigorous assessment of the use of ACTs in general, and AL in particular, for the treatment of P. vivax infections, either alone or in combination with primaquine, is merited. In the meantime, AL treatment of vivax malaria may be a pragmatic choice for areas with chloroquine-resistant P. vivax, and in co-endemic areas where AL is already used routinely against P. falciparum and parasitological differentiation is not routinely performed or only clinical diagnosis is used.
对于疟原虫中分布最广的间日疟原虫,人们对其了解甚少,这一情况亟待引起关注。人们越来越认识到这种寄生虫的真正负担及其在世界许多地区对氯喹(治疗间日疟的主要药物)产生耐药的可能性,这突显了确定新的有效治疗策略的必要性。青蒿素为基础的联合疗法(ACT)已被广泛用作治疗恶性疟原虫疟疾的一线药物,如果在疟疾和恶性疟原虫共同流行的地区使用,还将具有后勤方面的优势。然而,尽管 ACT 对恶性疟原虫的血期具有高且相似的疗效,但 ACT 和氯喹均不能有效对抗间日疟原虫休眠子,必须辅以全程使用伯氨喹才能根除休眠的间日疟原虫休眠子并预防复发。青蒿琥酯-咯萘啶(AL)是最常用的 ACT,它显示出快速清除间日疟原虫血症和退热的效果。与其他 ACT 相比,咯萘啶半衰期较短,这似乎有助于降低耐药风险。然而,它抑制间日疟复发或预防新感染的能力较短,这通常意味着体内短期疗效(例如,未校正的第 28 天或第 42 天治愈率)较低。假设不同的青蒿素衍生物对间日疟原虫具有等效疗效,那么 AL 与其他 ACT 之间的差异可能仅限于联合用药中另一药物的血浆治疗水平持续时间,这是一个具有有限临床意义的变量,特别是在低间日疟原虫传播率的地区,或者在添加伯氨喹预防复发的情况下。更严格地评估 ACT 一般,特别是 AL,单独或与伯氨喹联合用于治疗间日疟原虫感染是值得的。与此同时,在存在氯喹耐药间日疟原虫的地区,以及在间日疟原虫和恶性疟原虫共同流行的地区,AL 已经常规用于治疗恶性疟原虫,并且寄生虫学分化不是常规进行或仅使用临床诊断的情况下,AL 治疗间日疟可能是一种务实的选择。