Urologic Oncology Branch, the National Cancer Institute, Bethesda, MD, USA.
BJU Int. 2012 Jun;109(11):1600-6. doi: 10.1111/j.1464-410X.2011.10785.x. Epub 2012 Jan 5.
Study Type - Prognosis (case series) Level of Evidence 4 What's known on the subject? and What does the study add? Sarcomatoid renal cell carcinoma can occur in the setting of all histological subtypes of kidney cancer. These tumours are very aggressive and many patients present with disseminated disease. Long-term survival is poor and the durable responses to systemic therapy are infrequent. Our large cohort analyses the influence of pathological tumour characteristics in determining prognosis for patients with sarcomatoid renal cell carcinoma undergoing surgical resection. This series helps define the prognostic influence of histological subtype, type of sarcomatoid morphology, the percentage necrosis and sarcomatoid features, and the presence of microvascular invasion.
To examine the influence of pathological tumour characteristics on survival to aid prognostication and clinical trial design. Patients with sarcomatoid renal cell carcinoma (sRCC) are known to have poor prognosis and response to systemic therapy.
A single-centre database was reviewed to identify all patients with sRCC. Clinical variables and pathological information, including histology, necrosis, percentage of sarcomatoid features (PSF) and microvascular invasion (MVI), were recorded and correlated to outcome.
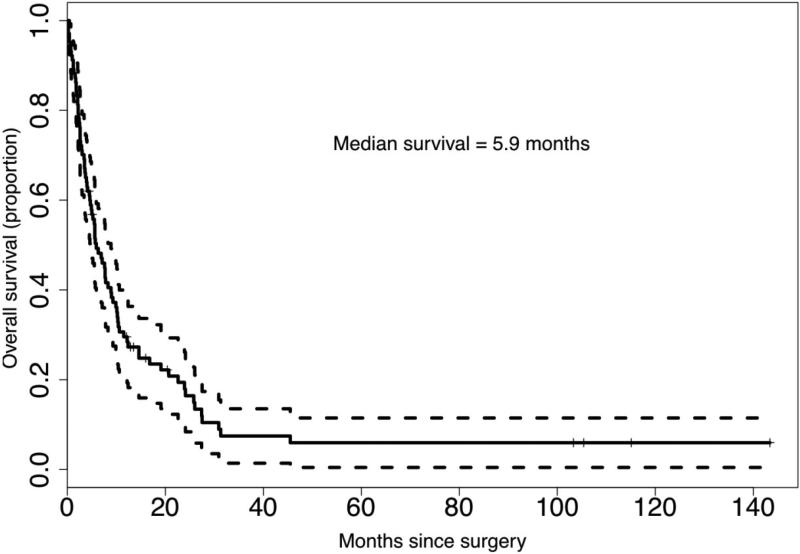
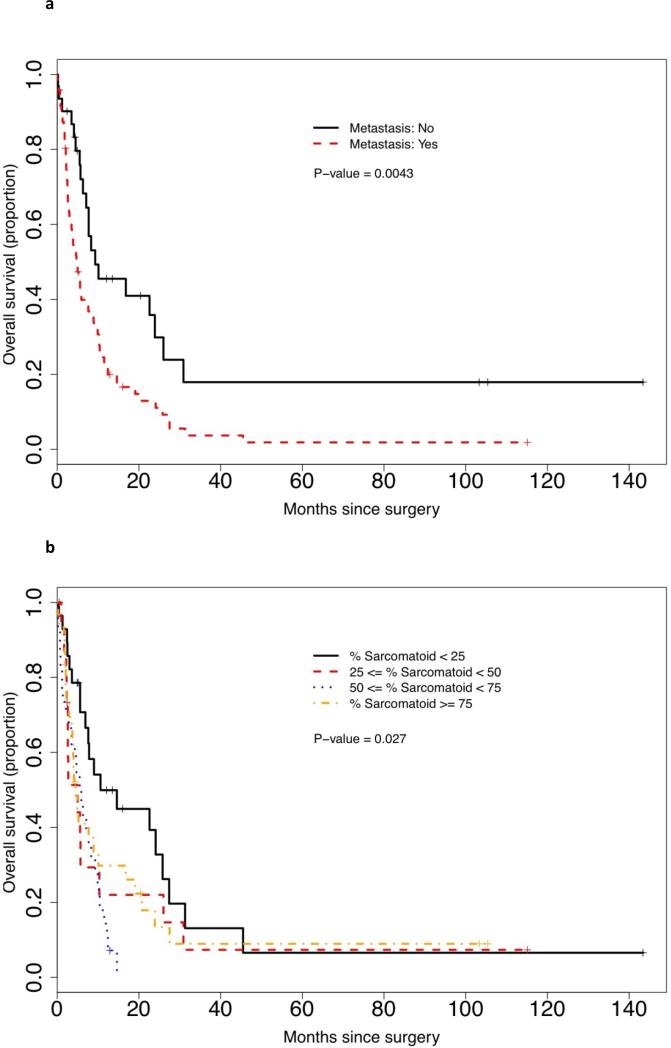
Analyses of 104 patients with sRCC found that the median (range) size of tumours was 9.5 cm (2.5-30), 65% of patients had areas of clear cell histology, and 69.2% had metastatic disease at presentation. The PSF did not influence tumour size, stage, necrosis, MVI, nodes or metastasis. A total of 85 patients (81.7%) died during the follow-up period with a median (95% confidence interval [CI]) survival of 5.9 months (4.7-8.9). In the overall cohort, Eastern Cooperative Group performance status (ECOGPS), tumour size and metastatic disease were independent predictors of poor survival. MVI, PSF and percentage necrosis were strongly associated with outcome but were not independent predictors of outcome. A multivariate risk model was established that incorporated six covariates (tumour size, MVI, ECOGPS, PSF, necrosis, and metastatic disease) to produce a predictive tool.
Both patients with localized and metastatic sRCC have very poor survival outcomes. Pathological features MVI, PSF and necrosis are important predictors of survival and could be used in a prognostic model while grade and histology do not influence prognosis. A prognostic model, if validated, could aid in patient counselling and/or clinical trial design.
探讨肿瘤病理特征对生存的影响,以辅助预后判断和临床试验设计。已知肉瘤样肾细胞癌(sRCC)患者预后差,对全身治疗反应差。
回顾性分析单中心数据库中所有 sRCC 患者的临床和病理资料,包括组织学、坏死、肉瘤样特征百分比(PSF)和微血管侵犯(MVI),并与预后相关联。
对 104 例 sRCC 患者的分析发现,肿瘤大小的中位数(范围)为 9.5cm(2.5-30),65%的患者有透明细胞组织学区域,69.2%的患者在就诊时已有转移病灶。PSF 不影响肿瘤大小、分期、坏死、MVI、淋巴结或转移。在随访期间,共有 85 例(81.7%)患者死亡,中位(95%置信区间[CI])生存时间为 5.9 个月(4.7-8.9)。在整个队列中,东部肿瘤协作组表现状态(ECOGPS)、肿瘤大小和转移性疾病是生存不良的独立预测因素。MVI、PSF 和坏死百分比与预后密切相关,但不是生存的独立预测因素。建立了一个多变量风险模型,该模型纳入了 6 个协变量(肿瘤大小、MVI、ECOGPS、PSF、坏死和转移性疾病),以生成一个预测工具。
局限性和转移性 sRCC 患者的生存结局均非常差。病理特征 MVI、PSF 和坏死是生存的重要预测因素,可用于预后模型,而分级和组织学不影响预后。如果验证有效,预后模型可辅助患者咨询和/或临床试验设计。