Department of Thoracic and Cardiovascular Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Korea.
World J Surg Oncol. 2012 Jan 12;10:9. doi: 10.1186/1477-7819-10-9.
We retrospectively reviewed the clinical features and surgical outcomes of patients with a surgically resected NSCLC invading chest wall in order to identify prognostic factors that impact long term survival.
Between January 1990 and December 2009, 107 patients who underwent surgical resection for chest wall invading NSCLC were reviewed. Tumors invading only the parietal pleura were defined as superficial invasions, and those involving the soft tissue or ribs were defined as deep invasions.
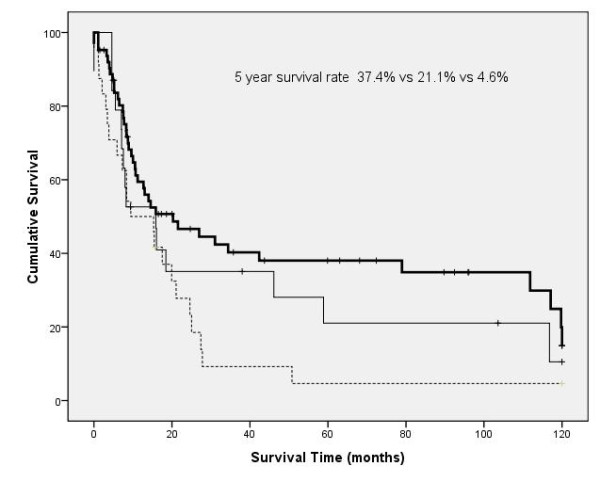
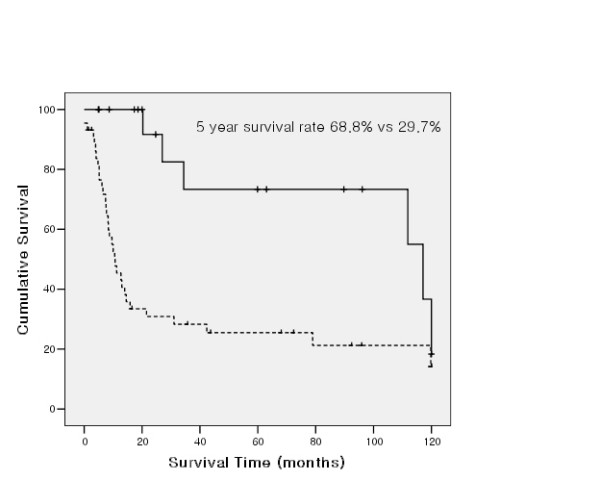
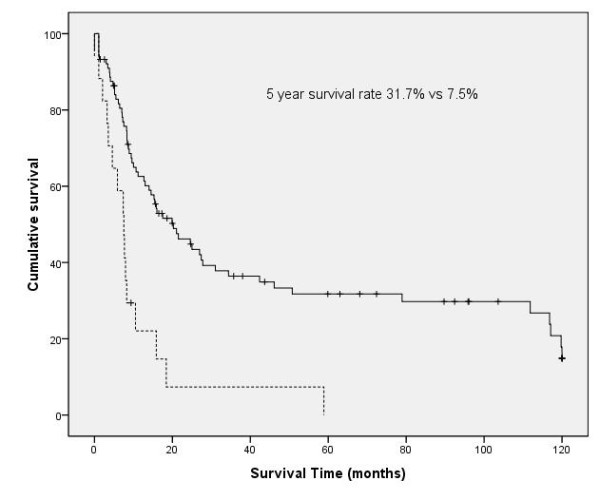
There were 91 men and 16 women; median age was 64 years (range 30 to 80 years). Overall 5 year survival rate was 26.3%. The univariate prognostic factors for survival included gender, extent of resection (pneumonectomy vs lobectomy), tumor size(> 5 cm vs ≤ 5 cm), nodal status (N0 or N1 vs N2), completeness of resection (complete vs incomplete) and completeness of adjuvant chemotherapy. At multivariate analysis, five independent prognostic factors were shown; depth of invasion (superficial vs deep), tumor size, nodal status, completeness of resection, and completeness of adjuvant chemotherapy. In patients with completely resected T3N0 NSCLC, completion of chemotherapy is the only prognostic factor for long term survival.
Completeness of resection, nodal status, depth of invasion, tumor size, and adjuvant chemotherapy were prognostic factors for long-term survival in NSCLC patients with chest wall invasion. Because of poor prognosis in cases with chest wall invasion that have N2 positive LN, that is difficult to achieve complete resection and that need pneumonectomy, definite chemoradiotherapy or neoadjuvant chemoradiotherapy should be considered first in these cases.
我们回顾性分析了手术切除的胸壁侵犯非小细胞肺癌(NSCLC)患者的临床特征和手术结果,以确定影响长期生存的预后因素。
1990 年 1 月至 2009 年 12 月,对 107 例接受手术切除胸壁侵犯 NSCLC 的患者进行了回顾性分析。仅侵犯壁层胸膜的肿瘤定义为浅表侵犯,累及软组织或肋骨的肿瘤定义为深部侵犯。
107 例患者中,男 91 例,女 16 例;中位年龄 64 岁(范围 30~80 岁)。总体 5 年生存率为 26.3%。单因素生存分析显示,影响生存的因素包括性别、切除范围(全肺切除术与肺叶切除术)、肿瘤大小(>5cm 与≤5cm)、淋巴结状态(N0 或 N1 与 N2)、切除完整性(完全与不完全)和辅助化疗的完整性。多因素分析显示,有 5 个独立的预后因素:侵犯深度(表浅与深部)、肿瘤大小、淋巴结状态、切除完整性和辅助化疗。在完全切除的 T3N0 NSCLC 患者中,完成化疗是长期生存的唯一预后因素。
在胸壁侵犯的 NSCLC 患者中,切除的完整性、淋巴结状态、侵犯深度、肿瘤大小和辅助化疗是影响长期生存的预后因素。由于胸壁侵犯伴 N2 阳性淋巴结的病例预后较差,难以达到完全切除且需要全肺切除术,这些病例应首先考虑明确的放化疗或新辅助放化疗。