School of Medicine, University of California, San Francisco, CA, USA.
BMC Public Health. 2012 Jan 12;12:30. doi: 10.1186/1471-2458-12-30.
While India has made significant progress in reducing maternal mortality, attaining further declines will require increased skilled birth attendance and institutional delivery among marginalized and difficult to reach populations.
A population-based survey was carried out among 16 randomly selected rural villages in rural Mysore District in Karnataka, India between August and September 2008. All households in selected villages were enumerated and women with children 6 years of age or younger underwent an interviewer-administered questionnaire on antenatal care and institutional delivery.
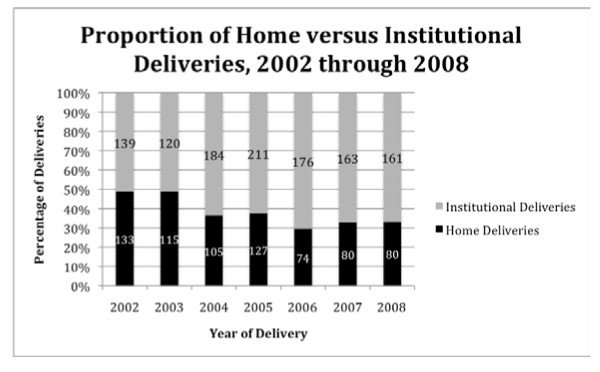
Institutional deliveries in rural areas of Mysore District increased from 51% to 70% between 2002 and 2008. While increasing numbers of women were accessing antenatal care and delivering in hospitals, large disparities were found in uptake of these services among different castes. Mothers belonging to general castes were almost twice as likely to have an institutional birth as compared to scheduled castes and tribes. Mothers belonging to other backward caste or general castes had 1.8 times higher odds (95% CI: 1.21, 2.89) of having an institutional delivery as compared to scheduled castes and tribes. In multivariable analysis, which adjusted for inter- and intra-village variance, Below Poverty Line status, caste, and receiving antenatal care were all associated with institutional delivery.
The results of the study suggest that while the Indian Government has made significant progress in increasing antenatal care and institutional deliveries among rural populations, further success in lowering maternal mortality will likely hinge on the success of NRHM programs focused on serving marginalized groups. Health interventions which target SC/ST may also have to address both perceived and actual stigma and discrimination, in addition to providing needed services. Strategies for overcoming these barriers may include sensitization of healthcare workers, targeted health education and outreach, and culturally appropriate community-level interventions. Addressing the needs of these communities will be critical to achieving Millennium Development Goal Five by 2015.
尽管印度在降低产妇死亡率方面取得了重大进展,但要进一步降低死亡率,就需要增加边缘化和难以接触到的人群中熟练的接生和住院分娩。
2008 年 8 月至 9 月,在印度卡纳塔克邦迈索尔区农村的 16 个随机选择的农村村庄进行了一项基于人群的调查。选择村庄中的所有家庭都进行了计数,并且有 6 岁或 6 岁以下儿童的妇女接受了访谈者管理的关于产前保健和住院分娩的问卷。
迈索尔区农村地区的住院分娩率从 2002 年的 51%增加到 2008 年的 70%。尽管越来越多的妇女接受产前保健并在医院分娩,但在不同种姓中,这些服务的利用率存在很大差异。一般种姓的母亲与在册种姓和部落相比,几乎有两倍的可能性进行住院分娩。与在册种姓和部落相比,其他落后种姓或一般种姓的母亲进行住院分娩的可能性要高出 1.8 倍(95%CI:1.21,2.89)。在调整村内和村间差异、贫困线以下状况、种姓和接受产前保健的多变量分析中,所有这些因素都与住院分娩有关。
研究结果表明,尽管印度政府在增加农村人口的产前保健和住院分娩方面取得了重大进展,但要进一步降低产妇死亡率,可能取决于印度国家农村健康计划在服务边缘化群体方面的成功。针对 SC/ST 的卫生干预措施也可能不仅要提供必要的服务,还要解决感知和实际的耻辱和歧视问题。克服这些障碍的策略可能包括提高卫生工作者的认识、有针对性的健康教育和外联,以及在文化上适当的社区一级干预。满足这些社区的需求对于到 2015 年实现千年发展目标五至关重要。