Public Health Foundation of India, Sector 44, Institutional Area, Gurugram, National Capital Region, India.
Institute for Health Metrics and Evaluation, University of Washington, Seattle, USA.
BMC Med. 2019 Jul 19;17(1):140. doi: 10.1186/s12916-019-1372-z.
The objectives of this study were to understand the differences in mortality rate, risk factors for mortality, and cause of death distribution in three neonatal age sub-groups (0-2, 3-7, and 8-27 days) and assess the change in mortality rate with previous assessments to inform programmatic decision-making in the Indian state of Bihar, a large state with a high burden of newborn deaths.
Detailed interviews were conducted in a representative sample of 23,602 live births between January and December 2016 (96.2% participation) in Bihar state. We estimated the neonatal mortality rate (NMR) for the three age sub-groups and explored the association of these deaths with a variety of risk factors using a hierarchical logistic regression model approach. Verbal autopsies were conducted using the PHMRC questionnaire and the cause of death assigned using the SmartVA automated algorithm. Change in NMR from 2011 to 2016 was estimated by comparing it with a previous assessment.
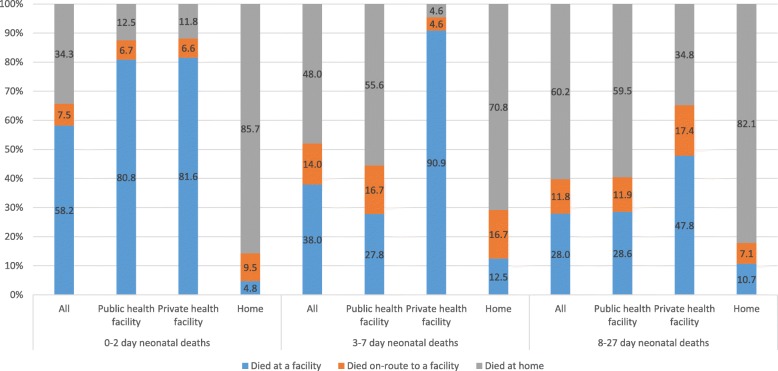
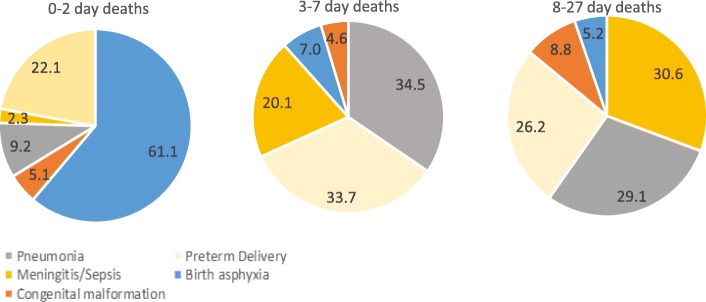
The NMR 0-2-day, 3-7-day, and 8-27-day mortality estimates in 2016 were 24.7 (95% CI 21.8-28.0), 13.2 (11.1 to 15.7), 5.8 (4.4 to 7.5), and 5.8 (4.5 to 7.5) per 1000 live births, respectively. A statistically significant reduction of 23.3% (95% CI 9.2% to 37.3) was seen in NMR from 2011 to 2016, driven by a reduction of 35.3% (95% CI 18.4% to 52.2) in 0-2-day mortality. In the final regression model, the highest odds for mortality in 0-2 days were related to the gestation period of ≤ 8 months (OR 16.5, 95% CI 11.9-22.9) followed by obstetric complications, no antiseptic cord care, and delivery at a private health facility or home. The 3-7- and 8-27-day mortality was driven by illness in the neonatal period (OR 10.33, 95% CI 6.31-16.90, and OR 4.88, 95% CI 3.13-7.61, respectively) and pregnancy with multiple foetuses (OR 5.15, 95% CI 2.39-11.10, and OR 11.77, 95% CI 6.43-21.53, respectively). Birth asphyxia (61.1%) and preterm delivery (22.1%) accounted for most of 0-2-day deaths; pneumonia (34.5%), preterm delivery (33.7%), and meningitis/sepsis (20.1%) accounted for the majority of 3-7-day deaths; meningitis/sepsis (30.6%), pneumonia (29.1%), and preterm delivery (26.2%) were the leading causes of death at 8-27 days.
To our knowledge, this is the first study to report a detailed neonatal epidemiology by age sub-groups for a major Indian state, which has highlighted the distinctly different mortality rate, risk factors, and causes of death at 0-2 days versus the rest of the neonatal period. Monitoring mortality at 0-2 and 3-7 days separately in the traditional early neonatal period of 0-7 days would enable more effective programming to reduce neonatal mortality.
本研究旨在了解三个新生儿年龄亚组(0-2 天、3-7 天和 8-27 天)的死亡率差异、死亡风险因素以及死亡原因分布,并评估死亡率的变化,以为印度比哈尔邦的规划决策提供信息,该邦是一个新生儿死亡负担较高的邦。
在比哈尔邦,我们对 2016 年 1 月至 12 月期间的 23602 例活产儿进行了有代表性的抽样调查(参与率为 96.2%),并对这三个年龄亚组的新生儿死亡率(NMR)进行了估计,并使用分层逻辑回归模型方法探讨了这些死亡与各种风险因素的关系。我们使用 PHMRC 问卷进行了口头尸检,并使用 SmartVA 自动算法确定了死亡原因。通过与前一次评估进行比较,估算了 2011 年至 2016 年期间 NMR 的变化。
2016 年,0-2 天、3-7 天和 8-27 天的 NMR 估计值分别为 24.7(95%CI 21.8-28.0)、13.2(11.1-15.7)、5.8(4.4-7.5)和 5.8(4.5-7.5)/1000 例活产儿。与 2011 年相比,2016 年的 NMR 下降了 23.3%(95%CI 9.2%-37.3%),这主要是由于 0-2 天死亡率下降了 35.3%(95%CI 18.4%-52.2%)。在最终的回归模型中,0-2 天死亡率最高的死亡风险因素与胎龄≤8 个月(OR 16.5,95%CI 11.9-22.9)、产科并发症、无消毒脐带护理以及在私立医疗机构或家中分娩有关。3-7 天和 8-27 天的死亡率与新生儿期的疾病(OR 10.33,95%CI 6.31-16.90,OR 4.88,95%CI 3.13-7.61)以及多胎妊娠(OR 5.15,95%CI 2.39-11.10,OR 11.77,95%CI 6.43-21.53)有关。出生窒息(61.1%)和早产(22.1%)是 0-2 天死亡的主要原因;肺炎(34.5%)、早产(33.7%)和脑膜炎/败血症(20.1%)是 3-7 天死亡的主要原因;脑膜炎/败血症(30.6%)、肺炎(29.1%)和早产(26.2%)是 8-27 天死亡的主要原因。
据我们所知,这是第一项针对印度主要邦的详细新生儿流行病学研究,该研究突出了 0-2 天与其余新生儿期之间明显不同的死亡率、风险因素和死亡原因。在传统的 0-7 天早期新生儿期分别监测 0-2 天和 3-7 天的死亡率,将有助于制定更有效的规划以降低新生儿死亡率。