Branch of Uterine Cancer, Research Institute and Hospital, National Cancer Center, Goyang, Korea.
J Gynecol Oncol. 2011 Dec;22(4):269-74. doi: 10.3802/jgo.2011.22.4.269. Epub 2011 Dec 5.
We aimed to determine the ideal cut-off of nadir serum CA-125 level for prediction of progression free survival.
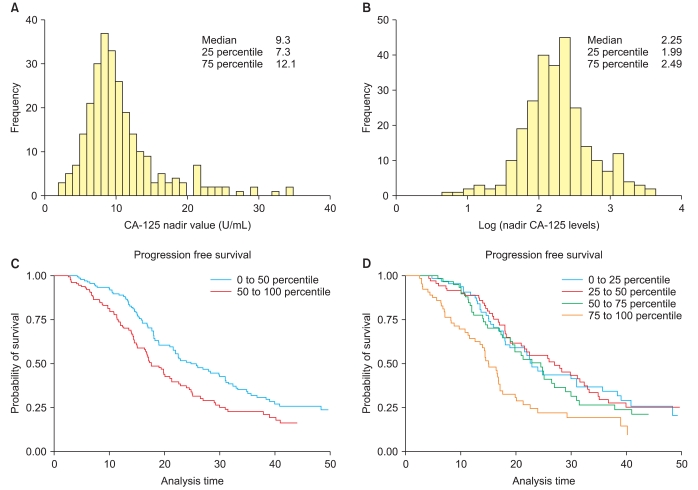
Among 267 patients who achieved complete remission after chemotherapy, the correlation between nadir CA-125 and progression free survival were compared among the subgroups classified according to the distribution of CA-125. The diagnostic odds ratio and area under the receiver operator characteristics curve were compared at various cut-off points.
The nadir CA-125 levels did not have prognostic value under 12 U/mL (to 75 percentile). In contrast, they were significantly correlated with progression free survival only when the CA-125 level was greater than 12, which was 75 percentile (p=0.034). In predicting progression free survival <6 and 12 months, the cut-off value of 18 (90 percentile) showed superior diagnostic performance over 10 or 12 U/mL. Compared with patients who showed nadir levels between 0 and 12 U/mL (0 to 75 percentile), those with nadir >18 U/mL showed a hazard ratio of 2.85 (95% confidence interval, 1.70 to 4.76; p<0.001); patients with nadir levels between 18 and 12 U/mL showed a the hazard ratio of 1.68 (95% confidence interval, 1.11 to 2.56; p=0.015) compared with those whose nadir levels were under 12 U/mL.
The predictive power of the traditional cut-off of 10 U/mL to classify a risk group or to identify high risk patients was unsatisfactory. The optimal diagnostic performance was observed at the cut-off of 18 U/mL and this can be proposed to dichotomize cut-off values to predict outcomes among individual patients.
我们旨在确定预测无进展生存期的血清 CA-125 水平最低值的理想切点。
在 267 例化疗后达到完全缓解的患者中,根据 CA-125 分布情况将患者分为亚组,比较各亚组 CA-125 最低值与无进展生存期的相关性。比较不同截断点下的诊断优势比和受试者工作特征曲线下面积。
CA-125 水平低于 12 U/mL(至 75 百分位)时,其无预后价值。相反,仅当 CA-125 水平大于 12 U/mL(75 百分位)时,CA-125 水平与无进展生存期显著相关(p=0.034)。在预测无进展生存期<6 个月和 12 个月时,18 U/mL(90 百分位)的截断值在诊断性能上优于 10 U/mL 或 12 U/mL。与 CA-125 水平在 0 至 12 U/mL(0 至 75 百分位)之间的患者相比,CA-125 水平低于 18 U/mL 的患者危险比为 2.85(95%置信区间,1.70 至 4.76;p<0.001);CA-125 水平在 18 至 12 U/mL 之间的患者的危险比为 1.68(95%置信区间,1.11 至 2.56;p=0.015),高于 CA-125 水平低于 12 U/mL 的患者。
传统截断值 10 U/mL 分类风险组或识别高危患者的预测能力并不令人满意。在截断值为 18 U/mL 时观察到最佳诊断性能,可建议将截断值二分法用于预测个体患者的结局。