Division of Cancer Epidemiology and Genetics, National Cancer Institute, Rockville, Maryland, United States of America.
PLoS One. 2012;7(1):e29051. doi: 10.1371/journal.pone.0029051. Epub 2012 Jan 13.
Cervical intraepithelial neoplasia grade 3 (CIN3), the immediate cervical cancer precursor, is a target of cervical cancer prevention. However, less than half of CIN3s will progress to cancer. Routine treatment of all CIN3s and the majority of CIN2s may lead to overtreatment of many lesions that would not progress. To improve our understanding of CIN3 natural history, we performed a detailed characterization of CIN3 heterogeneity in a large referral population in the US.
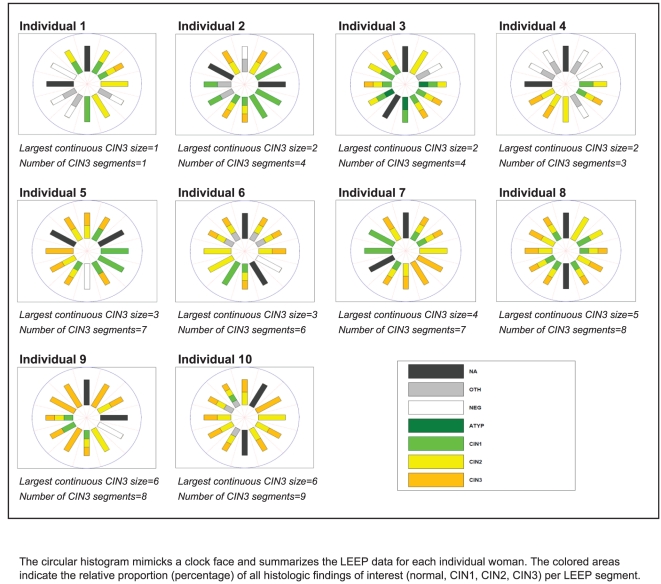
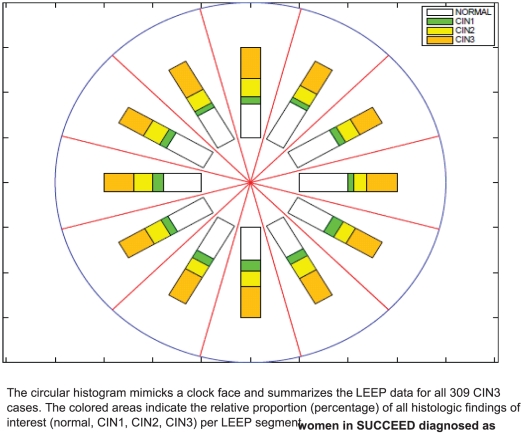
We examined 309 CIN3 cases in the SUCCEED, a large population-based study of women with abnormal cervical cancer screening results. Histology information for 12 individual loop electrosurgical excision procedure (LEEP) segments was evaluated for each woman. We performed case-case comparisons of CIN3s to analyze determinants of heterogeneity and screening test performance.
CIN3 cases varied substantially by size (1-10 LEEP segments) and by presentation with concomitant CIN2 and CIN1. All grades of CINs were equally distributed over the cervical surface. In half of the women, CIN3 lesions were found as multiple distinct lesions on the cervix. Women with large and solitary CIN3 lesions were more likely to be older, have longer sexual activity span, and have fewer multiple high risk HPV infections. Screening frequency, but not HPV16 positivity, was an important predictor of CIN3 size. Large CIN3 lesions were also characterized by high-grade clinical test results.
We demonstrate substantial heterogeneity in clinical and pathological presentation of CIN3 in a US population. Time since sexual debut and participation in screening were predictors of CIN3 size. We did not observe a preferential site of CIN3 on the cervical surface that could serve as a target for cervical biopsy. Cervical cancer screening procedures were more likely to detect larger CIN3s, suggesting that CIN3s detected by multiple independent diagnostic tests may represent cases with increased risk of invasion.
宫颈上皮内瘤变 3 级(CIN3)是宫颈癌的直接前体,是宫颈癌预防的目标。然而,不到一半的 CIN3 会发展为癌症。常规治疗所有 CIN3 和大多数 CIN2 可能导致对许多不会进展的病变的过度治疗。为了更好地了解 CIN3 的自然史,我们在美国的一个大型转诊人群中对 CIN3 的异质性进行了详细的描述。
我们对来自 SUCCEED 的 309 例 CIN3 病例进行了研究,这是一项针对宫颈癌筛查异常结果的女性的大型基于人群的研究。对每位女性的 12 个单独的环形电切术(LEEP)节段的组织学信息进行了评估。我们对 CIN3 病例进行了病例对照比较,以分析异质性的决定因素和筛查试验的性能。
CIN3 病例在大小(1-10 个 LEEP 节段)和同时伴有 CIN2 和 CIN1 的表现方面存在很大差异。所有级别的 CIN 均均匀分布在宫颈表面。在一半的女性中,CIN3 病变在宫颈上表现为多个不同的病变。CIN3 病变较大且为单发的女性年龄更大,性活动时间更长,且多次感染高危型 HPV 的情况较少。筛查频率,而不是 HPV16 阳性,是 CIN3 大小的重要预测因素。大的 CIN3 病变还具有高级别的临床检测结果。
我们在一个美国人群中证明了 CIN3 在临床和病理表现上存在很大的异质性。性活跃开始时间和参与筛查是 CIN3 大小的预测因素。我们没有观察到 CIN3 在宫颈表面的优先位置,这可能是宫颈活检的目标。宫颈癌筛查程序更有可能检测到较大的 CIN3,这表明通过多个独立诊断测试检测到的 CIN3 可能代表具有更高侵袭风险的病例。