Centre for Kidney Research, Children's Hospital at Westmead, Westmead, Australia.
PLoS One. 2012;7(1):e29591. doi: 10.1371/journal.pone.0029591. Epub 2012 Jan 18.
Deceased donor kidneys for transplantation are in most countries allocated preferentially to recipients who have limited co-morbidities. Little is known about the incremental health and economic gain from transplanting those with co-morbidities compared to remaining on dialysis. The aim of our study is to estimate the average and incremental survival benefits and health care costs of listing and transplantation compared to dialysis among individuals with varying co-morbidities.
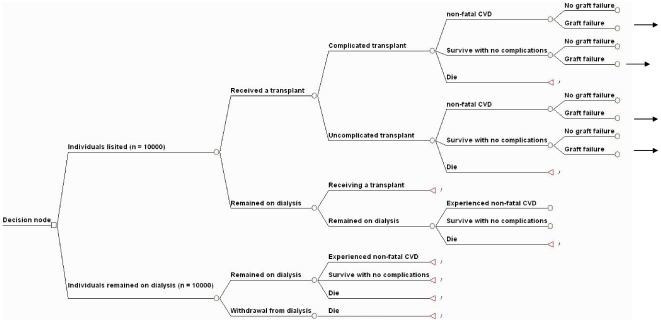
A probabilistic Markov model was constructed, using current outcomes for patients with defined co-morbidities treated with either dialysis or transplantation, to compare the health and economic benefits of listing and transplantation with dialysis.
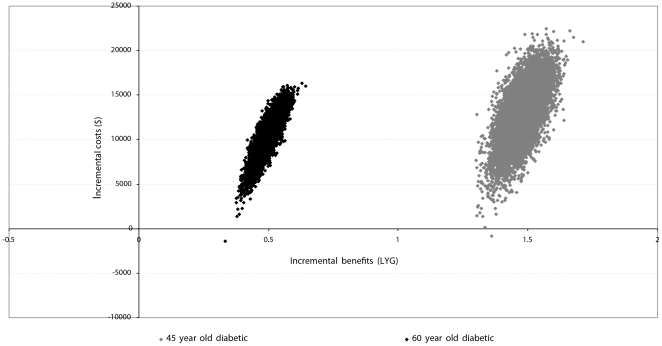
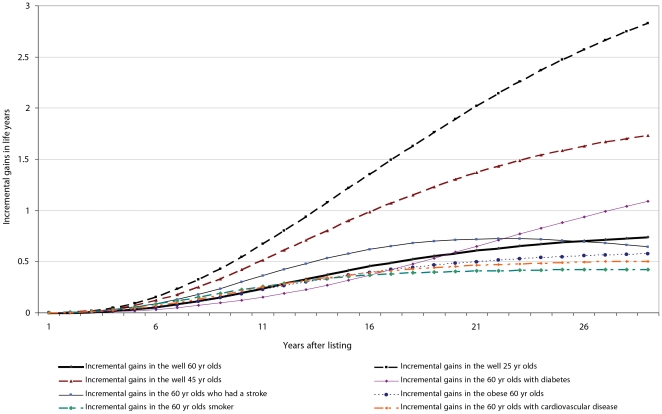
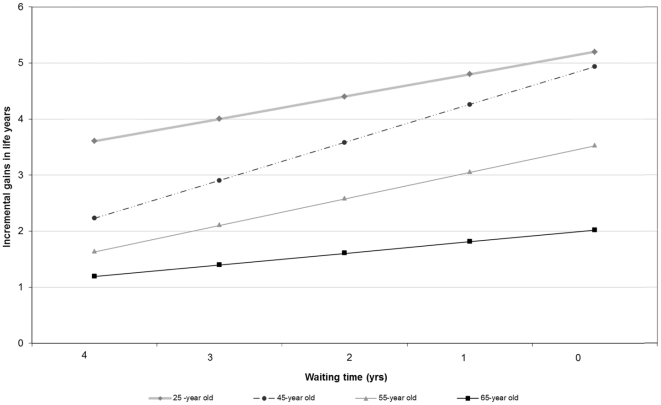
Using the current waiting time for deceased donor transplantation, transplanting a potential recipient, with or without co-morbidities achieves survival gains of between 6 months and more than three life years compared to remaining on dialysis, with an average incremental cost-effectiveness ratio (ICER) of less than $50,000/LYS, even among those with advanced age. Age at listing and the waiting time for transplantation are the most influential variables within the model. If there were an unlimited supply of organs and no waiting time, transplanting the younger and healthier individuals saves the most number of life years and is cost-saving, whereas transplanting the middle-age to older patients still achieves substantial incremental gains in life expectancy compared to being on dialysis.
Our modelled analyses suggest transplanting the younger and healthier individuals with end-stage kidney disease maximises survival gains and saves money. Listing and transplanting those with considerable co-morbidities is also cost-effective and achieves substantial survival gains compared with the dialysis alternative. Preferentially excluding the older and sicker individuals cannot be justified on utilitarian grounds.
在大多数国家,用于移植的已故供体肾脏优先分配给合并症有限的受者。与继续接受透析相比,将合并症患者移植的健康和经济效益增加情况知之甚少。我们的研究旨在评估在不同合并症患者中,与透析相比,列入名单和移植的平均和增量生存获益以及医疗保健成本。
使用接受透析或移植治疗的具有明确合并症的患者的当前结果,构建概率马尔可夫模型,以比较列入名单和移植与透析的健康和经济效益。
使用目前等待已故供体移植的时间,移植潜在受者,无论是否有合并症,与继续接受透析相比,可获得 6 个月至三年以上的生存获益,平均增量成本效益比(ICER)低于 50,000 美元/LYS,即使是在年龄较大的患者中也是如此。列入名单的年龄和等待移植的时间是模型内最具影响力的变量。如果器官供应无限且没有等待时间,那么移植年轻和健康的个体可以节省最多的生命年数,并且具有成本效益,而移植中年到老年患者与接受透析相比,仍能获得显著的预期寿命增量收益。
我们的模型分析表明,移植终末期肾病的年轻和健康个体可以最大限度地提高生存获益并节省资金。列入名单并移植合并症严重的患者也具有成本效益,与透析相比可获得显著的生存获益。基于功利主义理由,不能优先排除年龄较大和病情较重的患者。