Australian Center for Health Service Innovation, Queensland University of Technology, 60 Musk Ave, Kelvin Grove, QLD, 4059, Australia.
Royal Brisbane Hospital for Women, Brisbane, Australia.
BMC Health Serv Res. 2020 Oct 9;20(1):931. doi: 10.1186/s12913-020-05736-y.
Matching survival of a donor kidney with that of the recipient (longevity matching), is used in some kidney allocation systems to maximize graft-life years. It is not part of the allocation algorithm for Australia. Given the growing evidence of survival benefit due to longevity matching based allocation algorithms, development of a similar kidney allocation system for Australia is currently underway. The aim of this research is to estimate the impact that changes to costs and health outcomes arising from 'longevity matching' on the Australian healthcare system.
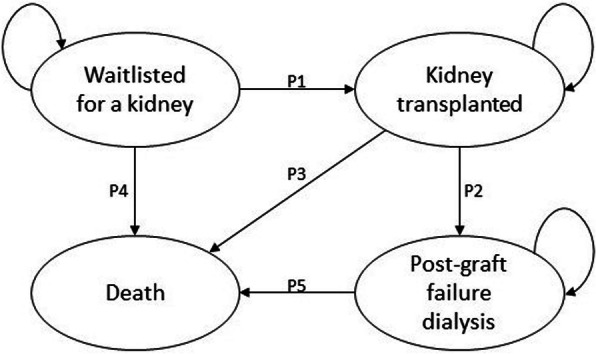
A decision analytic model to estimate cost-effectiveness was developed using a Markov process. Four plausible competing allocation options were compared to the current kidney allocation practice. Models were simulated in one-year cycles for a 20-year time horizon, with transitions through distinct health states relevant to the kidney recipient. Willingness to pay was considered as AUD 28000.
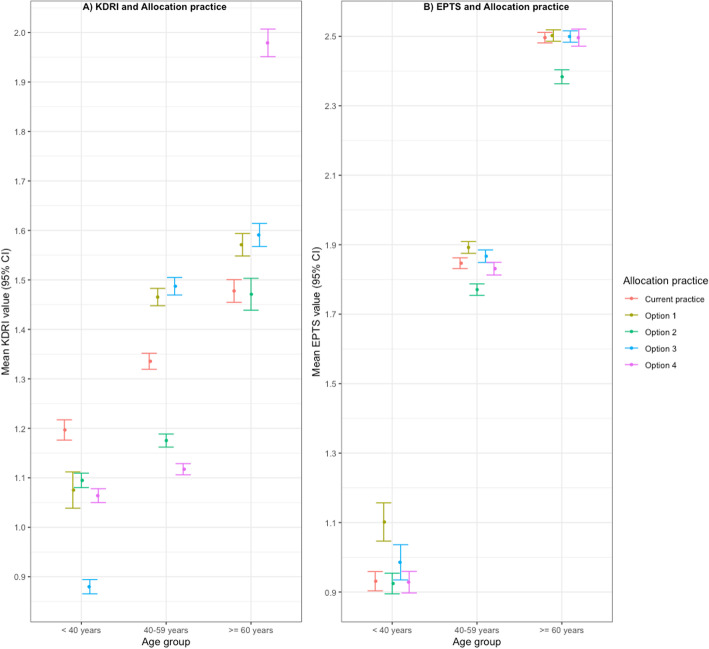
Base case analysis indicated that allocating the worst 20% of Kidney Donor Risk Index (KDRI) donor kidneys to the worst 20% of estimated post-transplant survival (EPTS) recipients (option 2) and allocating the oldest 25% of donor kidneys to the oldest 25% of recipients are both cost saving and more effective compared to the current Australian allocation practice. Option 2, returned the lowest costs, greatest health benefits and largest gain to net monetary benefits (NMB). Allocating the best 20% of KDRI donor kidneys to the best 20% of EPTS recipients had the lowest expected incremental NMB.
Of the four longevity-based kidney allocation practices considered, transplanting the lowest quality kidneys to the worst kidney recipients (option 2), was estimated to return the best value for money for the Australian health system.
在一些肾脏分配系统中,将供体肾脏的存活与受体的存活进行匹配(寿命匹配),以最大限度地延长移植物的寿命。它不是澳大利亚分配算法的一部分。鉴于基于寿命匹配的分配算法具有生存获益的证据越来越多,目前正在为澳大利亚开发类似的肾脏分配系统。本研究的目的是估计由于“寿命匹配”而导致成本和健康结果发生变化对澳大利亚医疗保健系统的影响。
使用马尔可夫过程开发了一种用于估计成本效益的决策分析模型。将四种可能的竞争性分配方案与当前的肾脏分配实践进行比较。模型在 20 年的时间范围内以一年为周期进行模拟,通过与肾脏受者相关的不同健康状态进行转换。考虑支付意愿为 28000 澳元。
基础案例分析表明,将最差的 20%的肾脏捐赠者风险指数(KDRI)供体肾脏分配给估计移植后存活最差的 20%的受者(方案 2),以及将最老的 25%的供体肾脏分配给最老的 25%的受者,与当前的澳大利亚分配实践相比,既节省成本又更有效。方案 2 成本最低,健康效益最大,净货币效益(NMB)增加最大。将 KDRI 供体肾脏的最佳 20%分配给 EPTS 受者的最佳 20%,其预期的增量 NMB 最低。
在所考虑的四种基于寿命的肾脏分配实践中,将质量最差的肾脏移植给最差的肾脏受者(方案 2),估计对澳大利亚卫生系统最具成本效益。