Department of Health Services Research and Policy, London School of Hygiene and Tropical Medicine, London, United Kingdom.
NHS Blood and Transplant, Bristol, United Kingdom.
Transplantation. 2020 Apr;104(4):795-803. doi: 10.1097/TP.0000000000002910.
The number of patients waiting to receive a kidney transplant outstrips the supply of donor organs. We sought to quantify trade-offs associated with different approaches to deceased donor kidney allocation in terms of quality-adjusted life years (QALYs), costs, and access to transplantation.
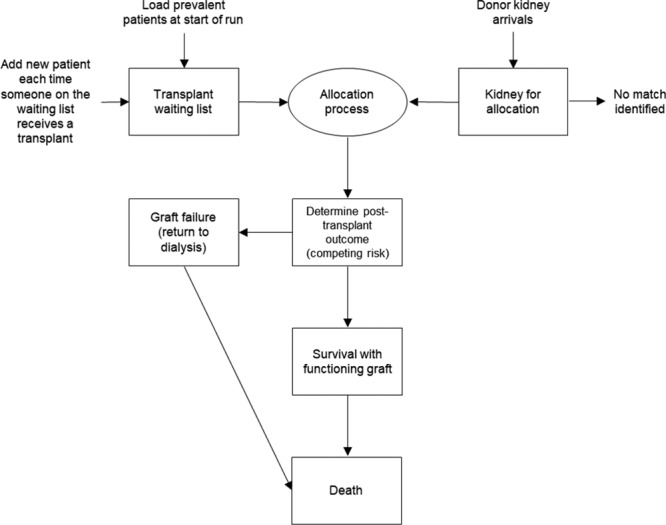
An individual patient simulation model was developed to compare 5 different approaches to kidney allocation, including the 2006 UK National Kidney Allocation Scheme (NKAS) and a QALY maximization approach designed to maximize health gains from a limited supply of donor organs. We used various sources of patient-level data to develop multivariable regression models to predict survival, health state utilities, and costs. We simulated the allocation of kidneys from 2200 deceased donors to a waiting list of 5500 patients and produced estimates of total lifetime costs and QALYs for each allocation scheme.
Among patients who received a transplant, the QALY maximization approach generated 48 045 QALYs and cost £681 million, while the 2006 NKAS generated 44 040 QALYs and cost £625 million. When also taking into consideration outcomes for patients who were not prioritized to receive a transplant, the 2006 NKAS produced higher total QALYs and costs and an incremental cost-effectiveness ratio of £110 741/QALY compared with the QALY maximization approach.
Compared with the 2006 NKAS, a QALY maximization approach makes more efficient use of deceased donor kidneys but reduces access to transplantation for older patients and results in greater inequity in the distribution of health gains between patients who receive a transplant and patients who remain on the waiting list.
等待接受肾移植的患者人数超过了可供捐赠器官的数量。我们旨在根据质量调整生命年(QALY)、成本和获得移植的机会来量化不同的已故供肾分配方法之间的权衡取舍。
我们开发了一个个体患者模拟模型,以比较 5 种不同的肾脏分配方法,包括 2006 年英国国家肾脏分配方案(NKAS)和旨在从有限的供体器官供应中最大化健康收益的 QALY 最大化方法。我们使用各种来源的患者水平数据来开发多变量回归模型,以预测生存、健康状态效用和成本。我们模拟了从 2200 名已故捐赠者向 5500 名等待名单患者分配肾脏,并为每种分配方案计算了总终身成本和 QALYs 的估计值。
在接受移植的患者中,QALY 最大化方法产生了 48045 个 QALY 和 6.81 亿英镑的成本,而 2006 年 NKAS 产生了 44040 个 QALY 和 6.25 亿英镑的成本。当还考虑到未被优先安排接受移植的患者的结果时,2006 年 NKAS 产生了更高的总 QALYs 和成本,以及与 QALY 最大化方法相比,增量成本效益比为 110741 英镑/QALY。
与 2006 年 NKAS 相比,QALY 最大化方法更有效地利用了已故供体的肾脏,但减少了老年患者的移植机会,并导致接受移植的患者和等待名单上的患者之间健康收益分配的更大不公平。