Department of Clinical Physiology, Skåne University Hospital, Lund University, Lund, Sweden.
J Cardiovasc Magn Reson. 2012 Jan 31;14(1):10. doi: 10.1186/1532-429X-14-10.
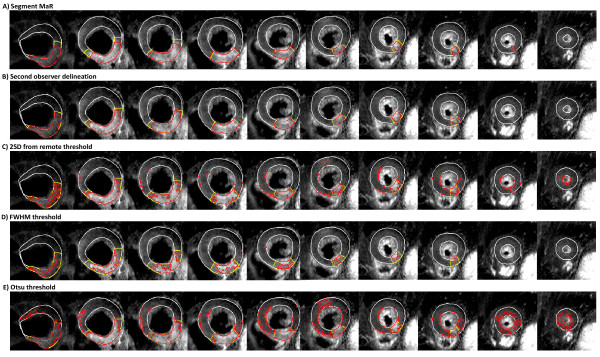
T2-weighted cardiovascular magnetic resonance (CMR) has been shown to be a promising technique for determination of ischemic myocardium, referred to as myocardium at risk (MaR), after an acute coronary event. Quantification of MaR in T2-weighted CMR has been proposed to be performed by manual delineation or the threshold methods of two standard deviations from remote (2SD), full width half maximum intensity (FWHM) or Otsu. However, manual delineation is subjective and threshold methods have inherent limitations related to threshold definition and lack of a priori information about cardiac anatomy and physiology. Therefore, the aim of this study was to develop an automatic segmentation algorithm for quantification of MaR using anatomical a priori information.
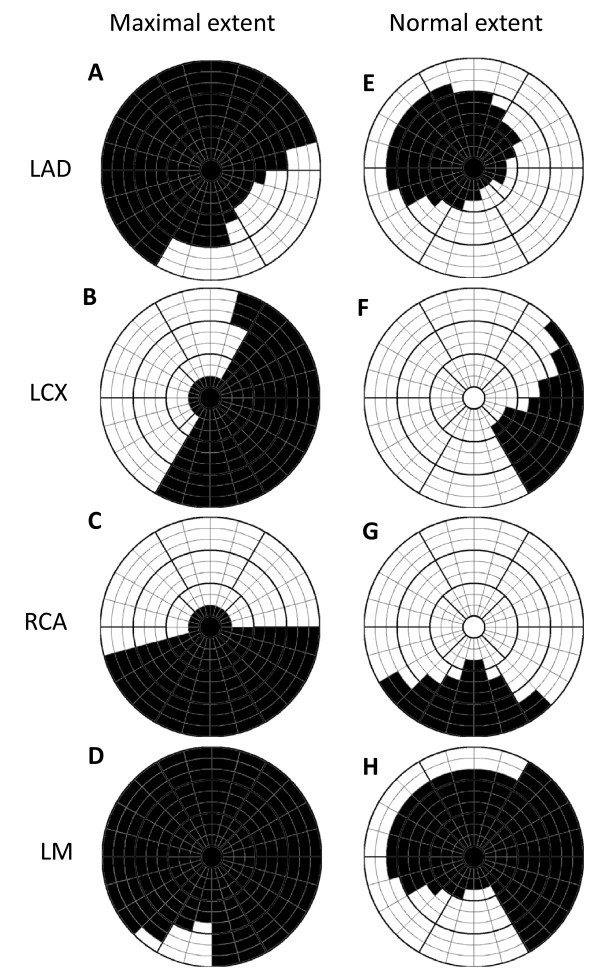
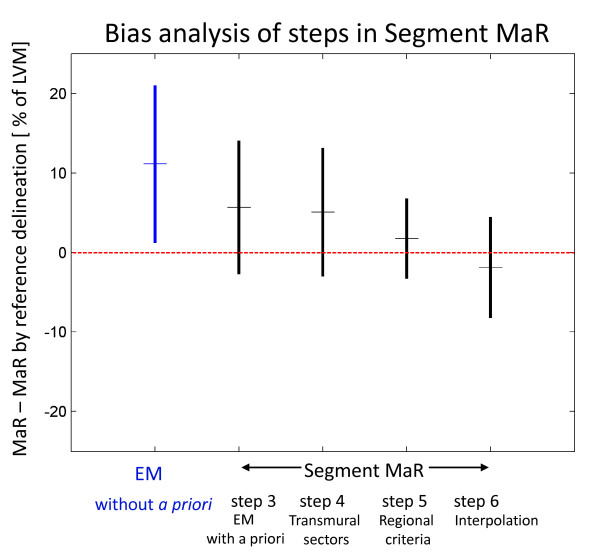
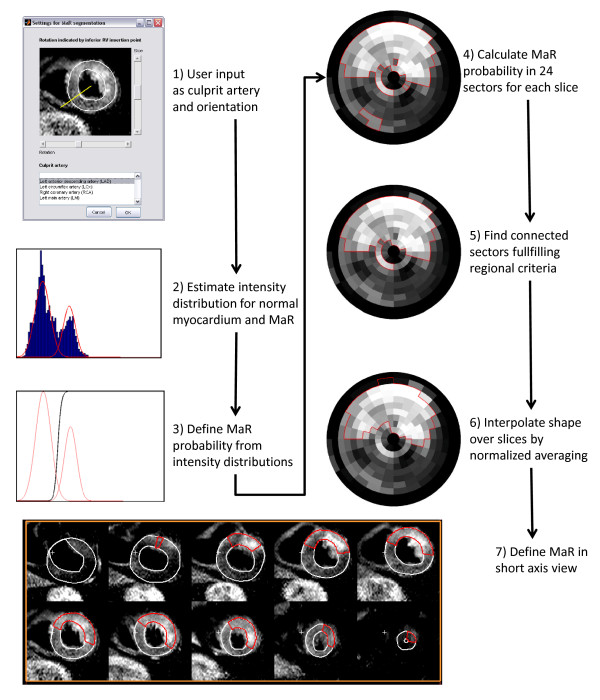
Forty-seven patients with first-time acute ST-elevation myocardial infarction underwent T2-weighted CMR within 1 week after admission. Endocardial and epicardial borders of the left ventricle, as well as the hyper enhanced MaR regions were manually delineated by experienced observers and used as reference method. A new automatic segmentation algorithm, called Segment MaR, defines the MaR region as the continuous region most probable of being MaR, by estimating the intensities of normal myocardium and MaR with an expectation maximization algorithm and restricting the MaR region by an a priori model of the maximal extent for the user defined culprit artery. The segmentation by Segment MaR was compared against inter observer variability of manual delineation and the threshold methods of 2SD, FWHM and Otsu.
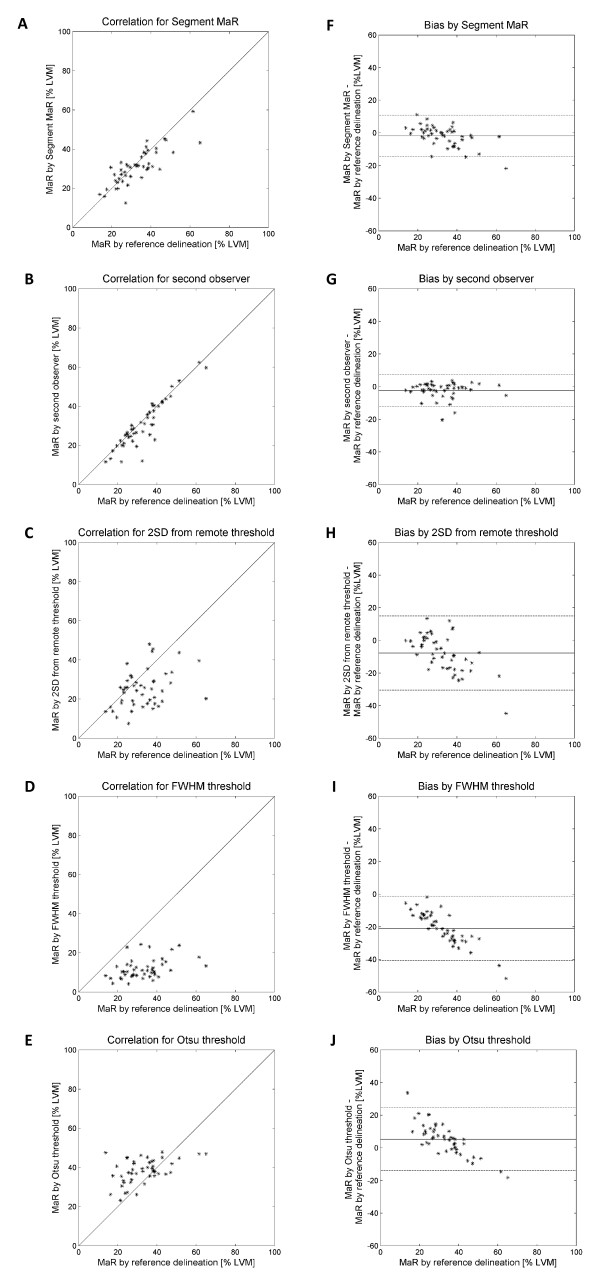
MaR was 32.9 ± 10.9% of left ventricular mass (LVM) when assessed by the reference observer and 31.0 ± 8.8% of LVM assessed by Segment MaR. The bias and correlation was, -1.9 ± 6.4% of LVM, R = 0.81 (p < 0.001) for Segment MaR, -2.3 ± 4.9%, R = 0.91 (p < 0.001) for inter observer variability of manual delineation, -7.7 ± 11.4%, R = 0.38 (p = 0.008) for 2SD, -21.0 ± 9.9%, R = 0.41 (p = 0.004) for FWHM, and 5.3 ± 9.6%, R = 0.47 (p < 0.001) for Otsu.
There is a good agreement between automatic Segment MaR and manually assessed MaR in T2-weighted CMR. Thus, the proposed algorithm seems to be a promising, objective method for standardized MaR quantification in T2-weighted CMR.
T2 加权心血管磁共振(CMR)已被证明是一种很有前途的技术,可用于确定急性冠状动脉事件后的缺血性心肌,即风险心肌(MaR)。T2 加权 CMR 中 MaR 的定量已被提议通过手动描绘或从远程(2SD)、全宽半最大值强度(FWHM)或 Otsu 的两个标准差的阈值方法进行。然而,手动描绘是主观的,而阈值方法具有与阈值定义相关的固有局限性,并且缺乏有关心脏解剖结构和生理学的先验信息。因此,本研究的目的是开发一种基于解剖学先验信息的自动分割算法,用于定量 MaR。
47 例首次急性 ST 段抬高型心肌梗死患者在入院后 1 周内行 T2 加权 CMR。左心室的心内膜和心外膜边界以及高强化 MaR 区域由经验丰富的观察者手动描绘,并作为参考方法使用。一种新的自动分割算法,称为 Segment MaR,通过估计正常心肌和 MaR 的强度,并通过用户定义的罪魁祸首动脉的最大范围的先验模型来限制 MaR 区域,将 MaR 区域定义为最有可能是 MaR 的连续区域。分割由 Segment MaR 与手动描绘的观察者间变异性和 2SD、FWHM 和 Otsu 的阈值方法进行比较。
参考观察者评估的 MaR 为左心室质量(LVM)的 32.9±10.9%,Segment MaR 评估的 MaR 为 31.0±8.8%LVM。Segment MaR 的偏倚和相关性为,-1.9±6.4%LVM,R=0.81(p<0.001);手动描绘的观察者间变异性为,-2.3±4.9%,R=0.91(p<0.001);2SD 为,-7.7±11.4%,R=0.38(p=0.008);FWHM 为,-21.0±9.9%,R=0.41(p=0.004);Otsu 为,5.3±9.6%,R=0.47(p<0.001)。
在 T2 加权 CMR 中,自动 Segment MaR 与手动评估的 MaR 之间具有良好的一致性。因此,该算法似乎是一种很有前途的、客观的 T2 加权 CMR 中标准化 MaR 定量方法。