Department of Neurosurgery, University of Münster, Albert-Schweitzer Campus 1, Geb. 1 A, 48149, Münster, Germany,
J Neurooncol. 2012 May;108(1):89-97. doi: 10.1007/s11060-012-0798-3. Epub 2012 Feb 4.
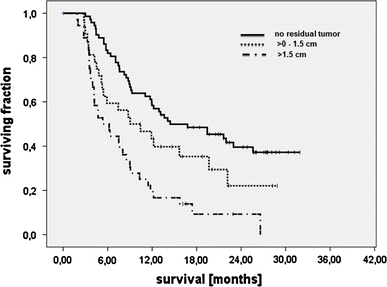
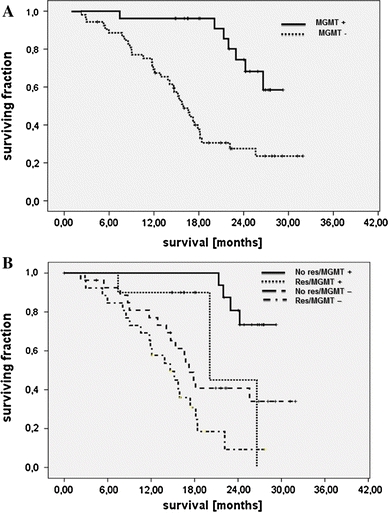
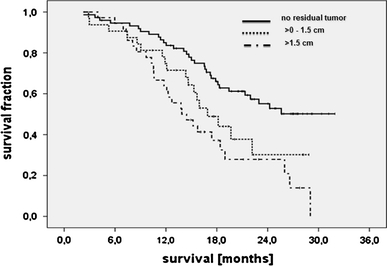
Survival of glioblastoma patients has been linked to the completeness of surgical resection. Available data, however, were generated with adjuvant radiotherapy. Data confirming that extensive cytoreduction remains beneficial to patients treated with the current standard, concomitant temozolomide radiochemotherapy, are limited. We therefore analyzed the efficacy of radiochemotherapy for patients with little or no residual tumor after surgery. In this prospective, non-interventional multicenter cohort study, entry criteria were histological diagnosis of glioblastoma, small enhancing or no residual tumor on post-operative MRI, and intended temozolomide radiochemotherapy. The primary study objective was progression-free survival; secondary study objectives were survival and toxicity. Furthermore, the prognostic value of O6-methylguanine-DNA methyltransferase (MGMT) promoter methylation was investigated in a subgroup of patients. One-hundred and eighty patients were enrolled. Fourteen were excluded by patient request or failure to initiate radiochemotherapy. Twenty-three patients had non-evaluable post-operative imaging. Thus, 143 patients qualified for analysis, with 107 patients having residual tumor diameters ≤1.5 cm. Median follow-up was 24.0 months. Median survival or patients without residual enhancing tumor exceeded the follow-up period. Median survival was 16.9 months for 32 patients with residual tumor diameters >0 to ≤1.5 cm (95% CI: 13.3-20.5, p = 0.039), and 13.9 months (10.3-17.5, overall p < 0.001) for 36 patients with residual tumor diameters >1.5 cm. Patient age at diagnosis and extent of resection were independently associated with survival. Patients with MGMT promoter methylated tumors and complete resection made the best prognosis. Completeness of resection acts synergistically with concomitant and adjuvant radiochemotherapy, especially in patients with MGMT promoter methylation.
胶质母细胞瘤患者的存活率与手术切除的完整性有关。然而,现有数据是在辅助放疗的情况下得出的。证实广泛细胞减灭术对接受当前标准治疗(同时给予替莫唑胺放化疗)的患者仍然有益的数据有限。因此,我们分析了手术后肿瘤残余很少或没有的患者接受放化疗的疗效。在这项前瞻性、非干预性多中心队列研究中,入组标准为组织学诊断为胶质母细胞瘤,术后 MRI 上肿瘤强化小或无残留肿瘤,且计划行替莫唑胺放化疗。主要研究终点为无进展生存期;次要研究终点为总生存期和毒性。此外,还在亚组患者中研究了 O6-甲基鸟嘌呤-DNA 甲基转移酶(MGMT)启动子甲基化的预后价值。共纳入 180 例患者。14 例患者因患者要求或未能开始放化疗而被排除。23 例患者术后影像学检查不可评估。因此,143 例患者符合分析条件,其中 107 例患者的肿瘤残余直径≤1.5cm。中位随访时间为 24.0 个月。无肿瘤残余增强的患者中位生存期超过随访期。32 例肿瘤残余直径>0 至≤1.5cm的患者中位生存期为 16.9 个月(95%CI:13.3-20.5,p=0.039),36 例肿瘤残余直径>1.5cm的患者中位生存期为 13.9 个月(10.3-17.5,总体 p<0.001)。诊断时的患者年龄和切除范围与生存独立相关。MGMT 启动子甲基化肿瘤和完全切除的患者预后最好。切除的完整性与同期和辅助放化疗协同作用,尤其是在 MGMT 启动子甲基化的患者中。