NHMRC Clinical Trials Centre, The University of Sydney, Sydney, Australia.
BMC Med Res Methodol. 2012 Feb 14;12:12. doi: 10.1186/1471-2288-12-12.
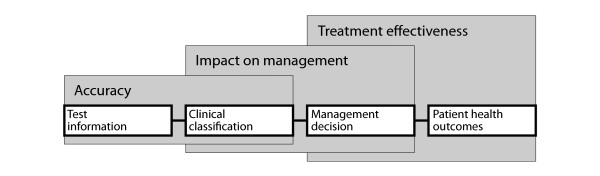
Before a new test is introduced in clinical practice, evidence is needed to demonstrate that its use will lead to improvements in patient health outcomes. Studies reporting test accuracy may not be sufficient, and clinical trials of tests that measure patient health outcomes are rarely feasible. Therefore, the consequences of testing on patient management are often investigated as an intermediate step in the pathway. There is a lack of guidance on the interpretation of this evidence, and patient management studies often neglect a discussion of the limitations of measuring patient management as a surrogate for health outcomes.
We discuss the rationale for measuring patient management, describe the common study designs and provide guidance about how this evidence should be reported.
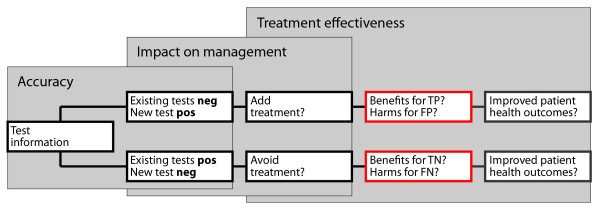
Interpretation of patient management studies relies on the condition that patient management is a valid surrogate for downstream patient benefits. This condition presupposes two critical assumptions: the test improves diagnostic accuracy; and the measured changes in patient management improve patient health outcomes. The validity of this evidence depends on the certainty around these critical assumptions and the ability of the study design to minimise bias. Three common designs are test RCTs that measure patient management as a primary endpoint, diagnostic before-after studies that compare planned patient management before and after testing, and accuracy studies that are extended to report on the actual treatment or further tests received following a positive and negative test result.
Patient management can be measured as a surrogate outcome for test evaluation if its limitations are recognised. The potential consequences of a positive and negative test result on patient management should be pre-specified and the potential patient benefits of these management changes clearly stated. Randomised comparisons will provide higher quality evidence about differences in patient management using the new test than observational studies. Regardless of the study design used, the critical assumption that patient management is a valid surrogate for downstream patient benefits or harms must be discussed in these studies.
在新的检验方法引入临床实践之前,需要有证据表明其使用将改善患者的健康结局。仅报告检验准确性的研究可能并不充分,且针对衡量患者健康结局的检验方法开展临床试验通常也不切实际。因此,检验对患者管理的影响往往作为该路径中的一个中间步骤进行研究。目前,对于该证据的解读缺乏指导,而患者管理研究往往忽略了衡量患者管理作为健康结局替代指标的局限性讨论。
我们讨论了衡量患者管理的基本原理,描述了常见的研究设计,并就如何报告此类证据提供了指导建议。
患者管理研究的解读依赖于以下假设,即患者管理是下游患者获益的有效替代指标。这一假设有两个关键前提:检验能提高诊断准确性;且测量的患者管理变化能改善患者的健康结局。该证据的有效性取决于这两个关键假设的确定性,以及研究设计最小化偏倚的能力。三种常见的设计包括:以患者管理为主要终点的检验随机对照试验;比较检验前后计划的患者管理的诊断前后研究;以及扩展以报告阳性和阴性检验结果后实际治疗或进一步检验的准确性研究。
如果认识到患者管理的局限性,其可以作为检验评估的替代结局进行测量。阳性和阴性检验结果对患者管理的潜在影响应预先设定,且明确说明这些管理变化对患者的潜在获益。与观察性研究相比,使用新检验方法进行的随机比较将为患者管理方面的差异提供更高质量的证据。无论使用何种研究设计,都必须在这些研究中讨论患者管理作为下游患者获益或危害的有效替代指标的关键假设。