Friesen Brendon R, Gibson Robert N, Speer Tony, Vincent Janette M, Stella Damien, Collier Neil A
Insights Imaging. 2011 Oct;2(5):525-531. doi: 10.1007/s13244-011-0100-9. Epub 2011 May 26.
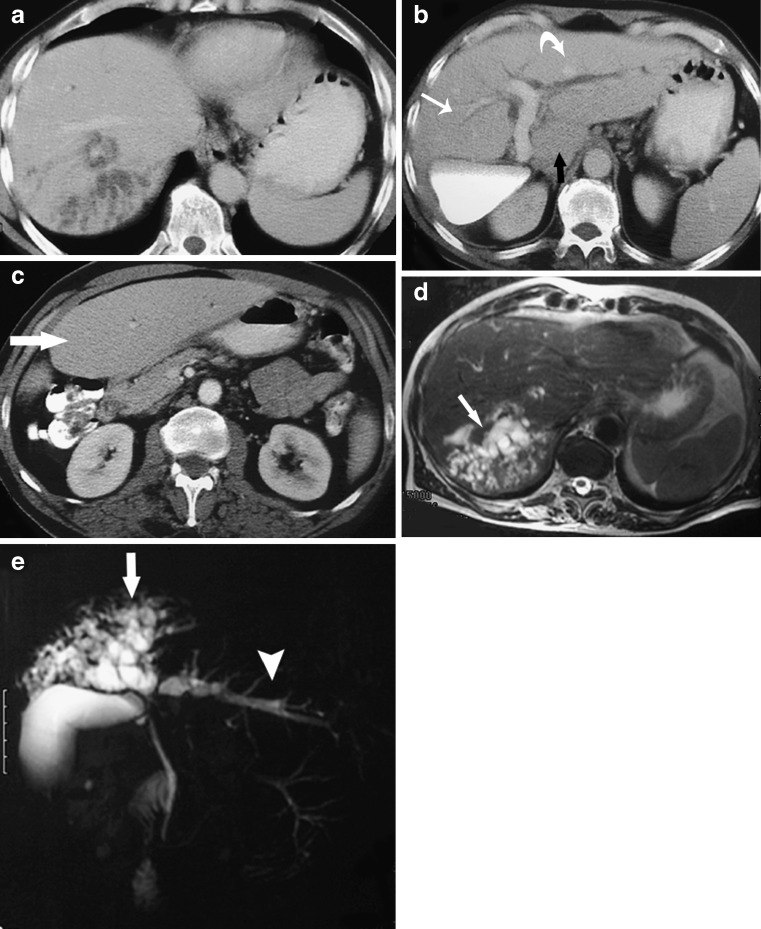
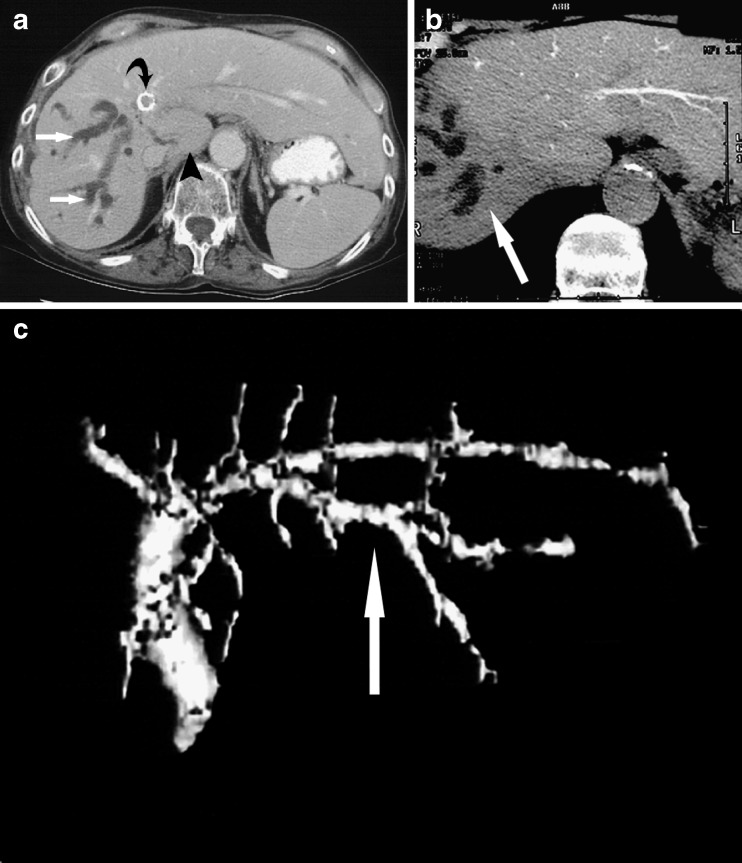
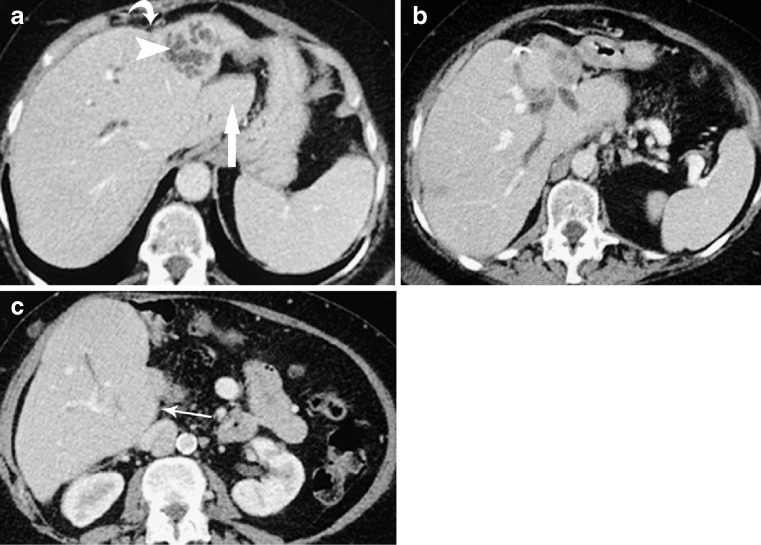
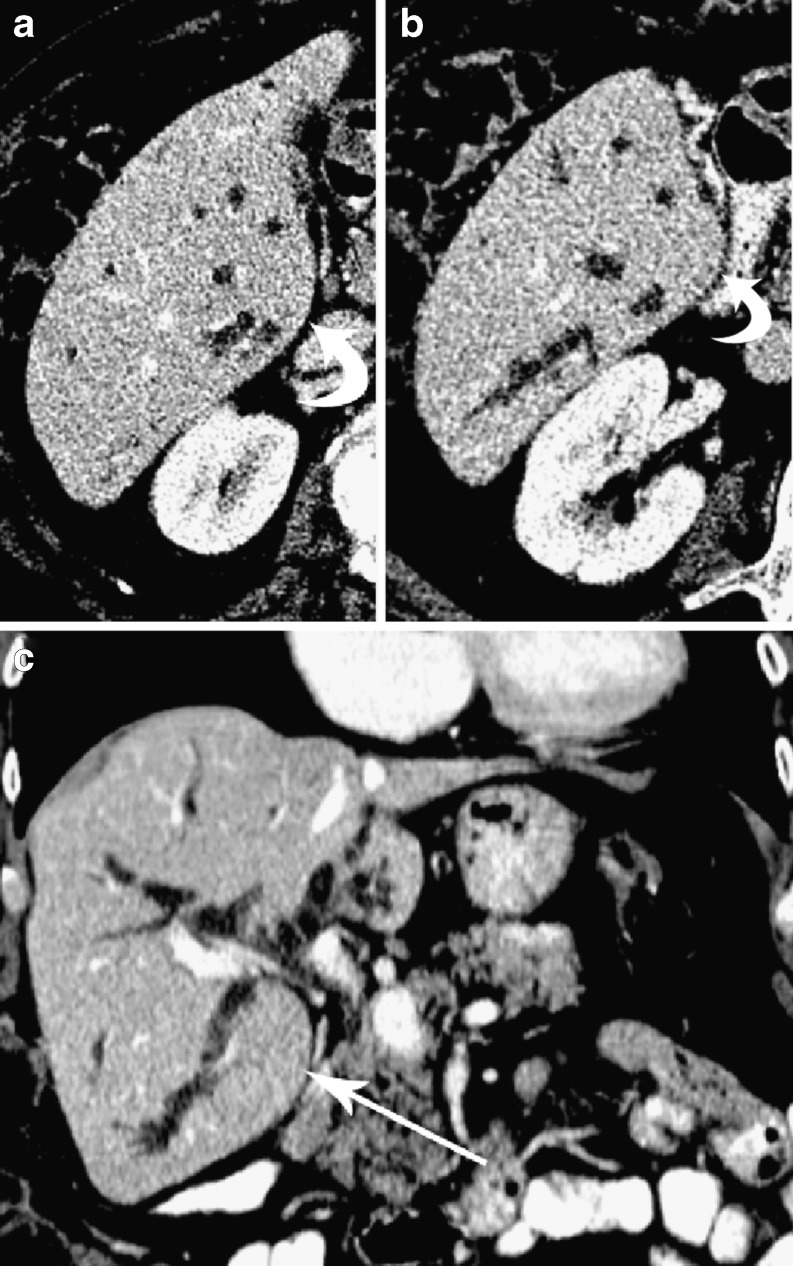
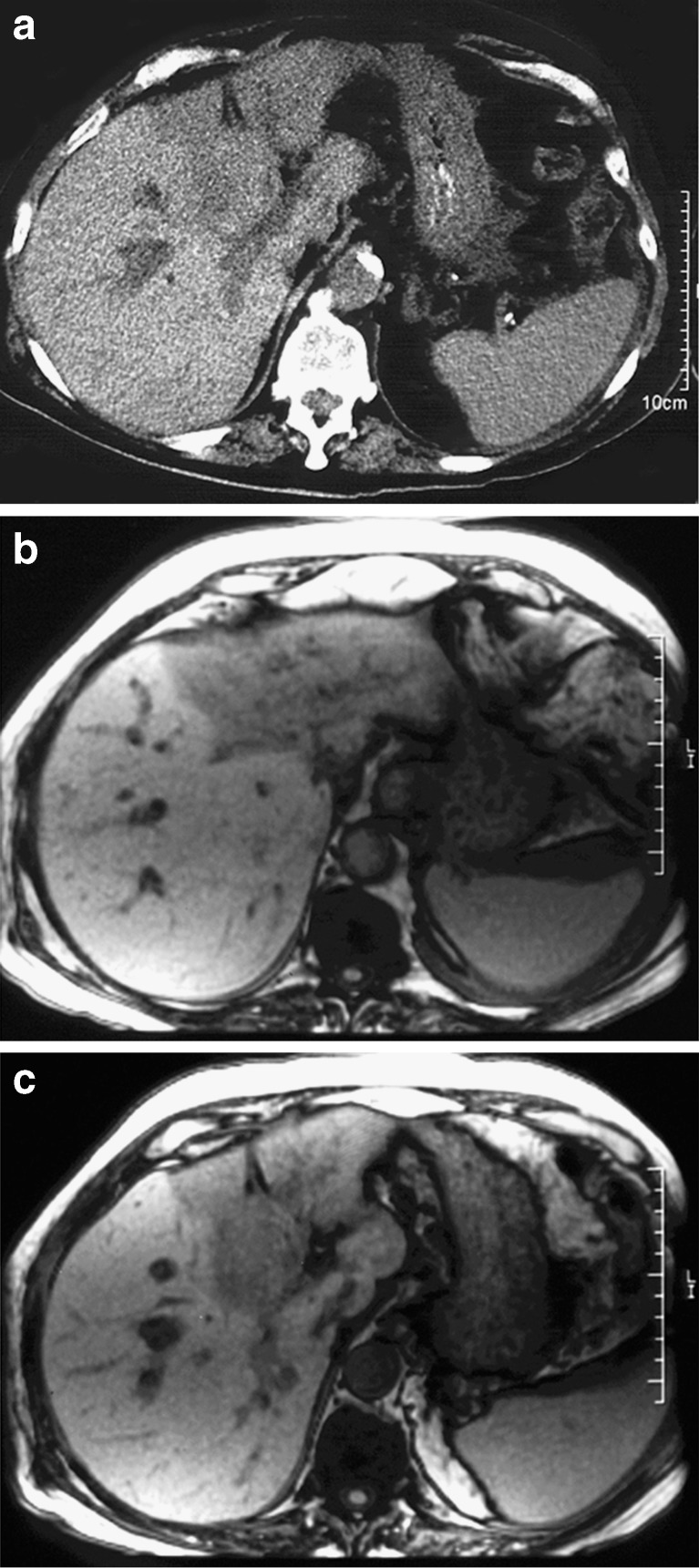
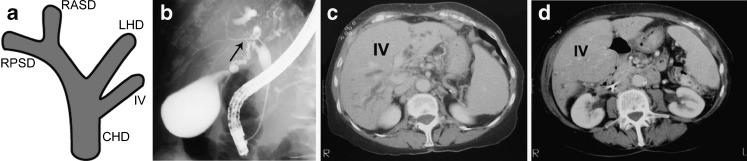
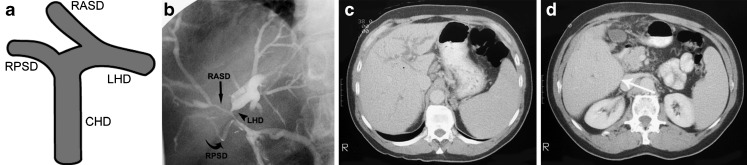
The radiological features of lobar and segmental liver atrophy and compensatory hypertrophy associated with biliary obstruction are important to recognise for diagnostic and therapeutic reasons. Atrophied lobes/segments reduce in volume and usually contain crowded dilated bile ducts extending close to the liver surface. There is often a "step" in the liver contour between the atrophied and non-atrophied parts. Hypertrophied right lobe or segments enlarge and show a prominently convex or "bulbous" visceral surface. The atrophied liver parenchyma may show lower attenuation on pre-contrast computed tomography (CT) and CT intravenous cholangiography (CT-IVC) and lower signal intensity on T1-weighted magnetic resonance imaging (MRI). Hilar biliary anatomical variants can have an impact on the patterns of lobar/segmental atrophy, as the cause of obstruction (e.g. cholangiocarcinoma) often commences in one branch, leading to atrophy in that drainage region before progressing to complete biliary obstruction and jaundice. Such variants are common and can result in unusual but explainable patterns of atrophy and hypertrophy. Examples of changes seen with and without hilar variants are presented that illustrate the radiological features of atrophy/hypertrophy.
认识与胆道梗阻相关的肝叶和肝段萎缩及代偿性肥大的放射学特征对于诊断和治疗具有重要意义。萎缩的肝叶/肝段体积减小,通常含有靠近肝表面延伸的密集扩张胆管。萎缩和未萎缩部分之间的肝脏轮廓常出现“台阶”。肥大的右叶或肝段增大,其脏面呈明显的凸面或“球根状”。萎缩的肝实质在对比剂增强前的计算机断层扫描(CT)和CT静脉胆管造影(CT-IVC)上可能显示较低的衰减,在T1加权磁共振成像(MRI)上显示较低的信号强度。肝门部胆道解剖变异可影响肝叶/肝段萎缩模式,因为梗阻原因(如胆管癌)通常始于一个分支,导致该引流区域萎缩,然后发展为完全性胆道梗阻和黄疸。此类变异很常见,可导致不寻常但可解释的萎缩和肥大模式。文中给出了有无肝门部变异时所见变化的实例,以说明萎缩/肥大的放射学特征。