Division of Pulmonology & UCT Lung Institute, Dept of Medicine, University of Cape Town, Cape Town, South Africa.
Eur Respir J. 2012 Nov;40(5):1211-20. doi: 10.1183/09031936.00201711. Epub 2012 Feb 23.
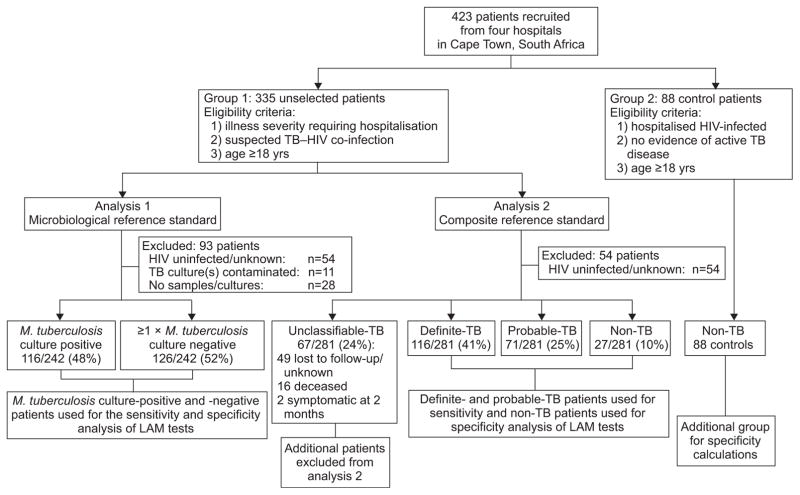
Lack of point-of-care tests for tuberculosis (TB) result in diagnostic delay, and increased mortality and healthcare-related costs. The urine Determine(TM) TB-LAM point-of-care strip-test was evaluated in 335 prospectively-recruited hospitalised patients with suspected TB-HIV co-infection (group 1) and from 88 HIV-infected hospitalised patients with non-TB diagnoses (group 2). Cut-off point-specific analyses were performed using: 1) a microbiological reference standard (culture positive versus negative); and 2) a composite reference standard (exclusion of patients with clinical-TB from the culture-negative group). Using the microbiological reference and the manufacturer-recommended grade-1 cut-off point, LAM sensitivity and specificity was 66% (95% CI 57-74%). By contrast, using the composite reference sensitivity was 60% (95% CI 53-67%) and specificity improved to 96% (95% CI 89-100%) (p=0.001). The same pattern was seen when the grade-2 cut-off point was used (specificity 75% versus 96%; p=0.01). In group two patients specificity was poor using the grade-1 cut-off point, but improved significantly when the grade-2 cut-off point was used (90% versus 99%; p=0.009). The grade-2 cut-off point also offered superior inter-reader reliability (p=0.002). Sensitivity was highest in those with a CD4 <200 cells per mL. LAM combined with smear-microscopy was able to rule-in TB in 71% of Mycobacterium tuberculosis culture-positive patients. This preliminary study indicates that the LAM strip-test may be a potentially useful rapid rule-in test for TB in hospitalised patients with advanced immunosuppression. The grade 2, but not the manufacturer-recommended grade 1 cut-off point, offered superior rule-in utility and inter-reader reliability. Larger studies to evaluate cut-off points and diagnostic accuracy are urgently required.
由于缺乏结核病(TB)的即时检测,导致诊断延迟,死亡率增加,以及医疗保健相关成本增加。在 335 名有疑似结核 - 艾滋病毒合并感染的住院患者(第 1 组)和 88 名患有非结核诊断的 HIV 感染住院患者(第 2 组)中评估了尿液 Determine(TM)TB-LAM 即时检测点检测。使用以下两种方法进行了基于截断值的分析:1)微生物学参考标准(培养阳性与阴性);2)综合参考标准(将培养阴性组中的临床结核患者排除在外)。使用微生物学参考标准和制造商推荐的 1 级截断值,LAM 的灵敏度和特异性为 66%(95%CI 57-74%)。相比之下,使用综合参考标准,灵敏度为 60%(95%CI 53-67%),特异性提高到 96%(95%CI 89-100%)(p=0.001)。当使用 2 级截断值时,也出现了相同的模式(特异性为 75%与 96%;p=0.01)。在第 2 组患者中,使用 1 级截断值时特异性较差,但使用 2 级截断值时显著提高(90%与 99%;p=0.009)。2 级截断值还提供了更好的读者间可靠性(p=0.002)。在 CD4 细胞<200 个/毫升的患者中,灵敏度最高。LAM 与涂片显微镜检查相结合,能够在 71%的结核分枝杆菌培养阳性患者中确诊 TB。这项初步研究表明,LAM 条带检测可能是一种有潜在价值的快速诊断工具,用于诊断住院患者中晚期免疫抑制相关的结核病。2 级截断值(而不是制造商推荐的 1 级截断值)提供了更好的纳入标准效用和读者间可靠性。迫切需要进行更大规模的研究来评估截断值和诊断准确性。