Division of Global HIV and TB, Centers for Disease Control and Prevention, Atlanta, Georgia, USA.
Avenir Health, Glastonbury, Connecticut, USA.
J Int AIDS Soc. 2023 Mar;26(3):e26070. doi: 10.1002/jia2.26070.
Despite antiretroviral therapy (ART) scale-up among people living with HIV (PLHIV), those with advanced HIV disease (AHD) (defined in adults as CD4 count <200 cells/mm or clinical stage 3 or 4), remain at high risk of death from opportunistic infections. The shift from routine baseline CD4 testing towards viral load testing in conjunction with "Test and Treat" has limited AHD identification.
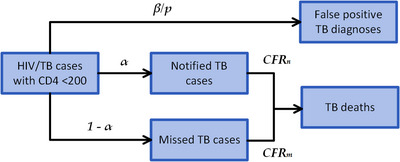
We used official estimates and existing epidemiological data to project deaths from tuberculosis (TB) and cryptococcal meningitis (CM) among PLHIV-initiating ART with CD4 <200 cells/mm , in the absence of select World Health Organization recommended diagnostic or therapeutic protocols for patients with AHD. We modelled the reduction in deaths, based on the performance of screening/diagnostic testing and the coverage and efficacy of treatment/preventive therapies for TB and CM. We compared projected TB and CM deaths in the first year of ART from 2019 to 2024, with and without CD4 testing. The analysis was performed for nine countries: South Africa, Kenya, Lesotho, Mozambique, Nigeria, Uganda, Zambia, Zimbabwe and the Democratic Republic of Congo.
The effect of CD4 testing comes through increased identification of AHD and consequent eligibility for protocols for AHD prevention, diagnosis and management; algorithms for CD4 testing avert between 31% and 38% of deaths from TB and CM in the first year of ART. The number of CD4 tests required per death averted varies widely by country from approximately 101 for South Africa to 917 for Kenya.
This analysis supports retaining baseline CD4 testing to avert deaths from TB and CM, the two most deadly opportunistic infections among patients with AHD. However, national programmes will need to weigh the cost of increasing CD4 access against other HIV-related priorities and allocate resources accordingly.
尽管抗逆转录病毒疗法(ART)在艾滋病毒感染者(PLHIV)中得到了普及,但那些患有晚期 HIV 疾病(AHD)的人(在成年人中定义为 CD4 计数<200 个细胞/mm 或临床阶段 3 或 4)仍然面临因机会性感染而死亡的高风险。从常规的基线 CD4 检测转向与“检测即治疗”相结合的病毒载量检测,限制了对 AHD 的识别。
我们使用官方估计和现有流行病学数据,在没有针对 AHD 患者的世界卫生组织推荐的诊断或治疗方案的情况下,对 CD4<200 个细胞/mm 的开始接受 ART 的 PLHIV 死于结核病(TB)和隐球菌性脑膜炎(CM)的情况进行了预测。我们根据筛查/诊断检测的性能以及 TB 和 CM 的治疗/预防疗法的覆盖率和疗效,对死亡人数的减少进行了建模。我们比较了 2019 年至 2024 年期间,在没有和有 CD4 检测的情况下,ART 第一年的预期 TB 和 CM 死亡人数。分析针对九个国家进行:南非、肯尼亚、莱索托、莫桑比克、尼日利亚、乌干达、赞比亚、津巴布韦和刚果民主共和国。
CD4 检测的效果是通过增加对 AHD 的识别,以及随后获得 AHD 预防、诊断和管理方案的资格来实现的;CD4 检测算法在 ART 的第一年避免了 31%至 38%的 TB 和 CM 死亡。每个避免的死亡所需的 CD4 检测数量因国家而异,从南非的约 101 次到肯尼亚的 917 次不等。
这项分析支持保留基线 CD4 检测,以避免 AHD 患者死于 TB 和 CM,这两种是 AHD 患者中最致命的机会性感染。然而,国家规划者需要权衡增加 CD4 检测的成本与其他与 HIV 相关的优先事项,并相应地分配资源。