Centre for Endocrinology, Diabetes and Metabolism, Institute of Biomedical Research, School of Clinical and Experimental Medicine, University of Birmingham, Birmingham, United Kingdom.
PLoS One. 2012;7(2):e29531. doi: 10.1371/journal.pone.0029531. Epub 2012 Feb 20.
Non alcoholic fatty liver disease (NAFLD) is the hepatic manifestation of the metabolic syndrome. NAFLD represents a spectrum of liver disease ranging from reversible hepatic steatosis, to non alcoholic steato-hepatitis (NASH) and cirrhosis. The potential role of glucocorticoids (GC) in the pathogenesis of NAFLD is highlighted in patients with GC excess, Cushing's syndrome, who develop central adiposity, insulin resistance and in 20% of cases, NAFLD. Although in most cases of NAFLD, circulating cortisol levels are normal, hepatic cortisol availability is controlled by enzymes that regenerate cortisol (F) from inactive cortisone (E) (11β-hydroxysteroid dehydrogenase type 1, 11β-HSD1), or inactivate cortisol through A-ring metabolism (5α- and 5β-reductase, 5αR and 5βR).
In vitro studies defined 11β-HSD1 expression in normal and NASH liver samples. We then characterised hepatic cortisol metabolism in 16 patients with histologically proven NAFLD compared to 32 obese controls using gas chromatographic analysis of 24 hour urine collection and plasma cortisol generation profile following oral cortisone.
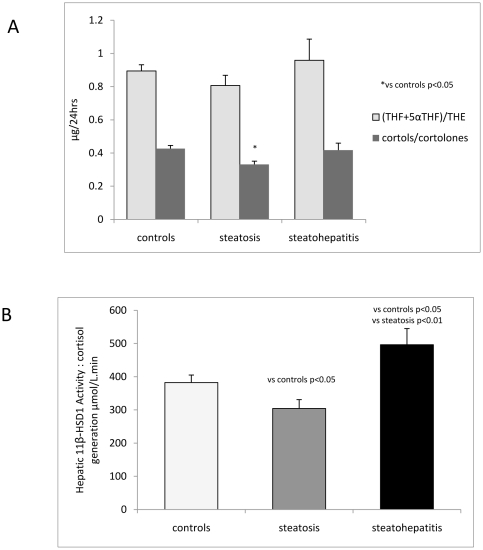
In patients with steatosis 5αR activity was increased, with a decrease in hepatic 11β-HSD1 activity. Total cortisol metabolites were increased in this group consistent with increased GC production rate. In contrast, in patients with NASH, 11β-HSD1 activity was increased both in comparison to patients with steatosis, and controls. Endorsing these findings, 11β-HSD1 mRNA and immunostaining was markedly increased in NASH patients in peri septal hepatocytes and within CD68 positive macrophages within inflamed cirrhotic septa.
Patients with hepatic steatosis have increased clearance and decreased hepatic regeneration of cortisol and we propose that this may represent a protective mechanism to decrease local GC availability to preserve hepatic metabolic phenotype. With progression to NASH, increased 11β-HSD1 activity and consequent cortisol regeneration may serve to limit hepatic inflammation.
非酒精性脂肪性肝病(NAFLD)是代谢综合征的肝脏表现。NAFLD 代表了一系列从可逆性肝脂肪变性到非酒精性脂肪性肝炎(NASH)和肝硬化的肝脏疾病谱。糖皮质激素(GC)在 NAFLD 发病机制中的潜在作用在 GC 过多的患者中得到强调,如库欣综合征患者,他们会出现中心性肥胖、胰岛素抵抗,并且在 20%的情况下出现 NAFLD。尽管在大多数 NAFLD 病例中,循环皮质醇水平正常,但肝脏皮质醇的可用性受将无活性可的松(E)转化为皮质醇(F)的酶(11β-羟类固醇脱氢酶 1 型,11β-HSD1)或通过 A 环代谢使皮质醇失活(5α-和 5β-还原酶,5αR 和 5βR)控制。
体外研究定义了正常和 NASH 肝组织样本中的 11β-HSD1 表达。然后,我们使用气相色谱分析 24 小时尿液收集和口服皮质醇后的血浆皮质醇生成谱,比较了 16 例经组织学证实的 NAFLD 患者与 32 例肥胖对照者的肝皮质醇代谢。
在脂肪变性患者中,5αR 活性增加,而肝 11β-HSD1 活性降低。该组的总皮质醇代谢物增加,与 GC 生成率增加一致。相比之下,在 NASH 患者中,11β-HSD1 活性与脂肪变性患者和对照组相比均增加。这些发现的佐证是,在 NASH 患者的周细胞和炎症性肝间隔内的 CD68 阳性巨噬细胞中,11β-HSD1mRNA 和免疫染色明显增加。
肝脂肪变性患者的皮质醇清除率增加,肝内皮质醇再生减少,我们认为这可能是一种保护机制,以减少局部 GC 可用性,以维持肝代谢表型。随着 NASH 的进展,增加的 11β-HSD1 活性和随之而来的皮质醇再生可能有助于限制肝炎症。