Global Medicines Program, Department of Global Health, School of Public Health, University of Washington, Seattle, Washington, United States of America.
PLoS One. 2012;7(2):e30735. doi: 10.1371/journal.pone.0030735. Epub 2012 Feb 17.
Over two thirds of women who need contraception in Uganda lack access to modern effective methods. This study was conducted to estimate the potential cost-effectiveness of achieving universal access to modern contraceptives in Uganda by implementing a hypothetical new contraceptive program (NCP) from both societal and governmental (Ministry of Health (MoH)) perspectives.
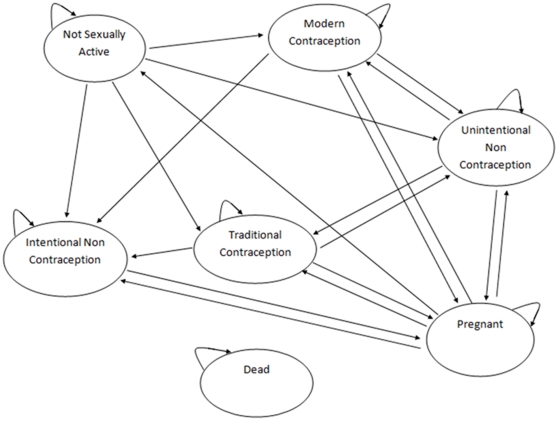
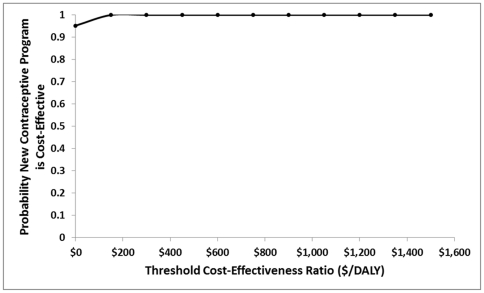
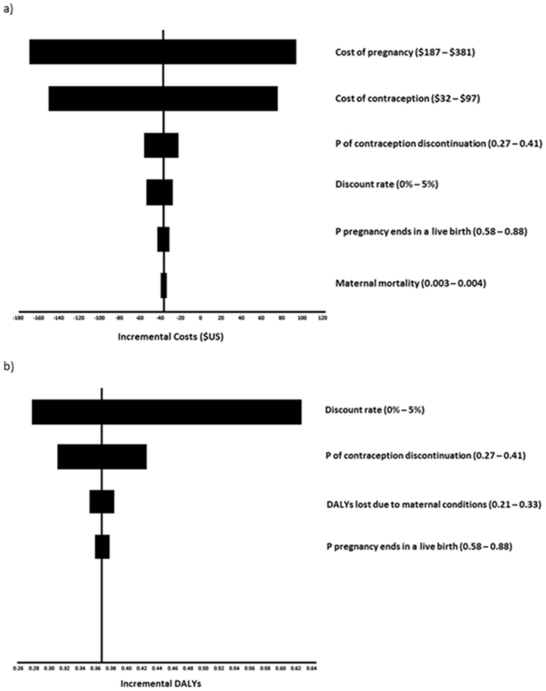
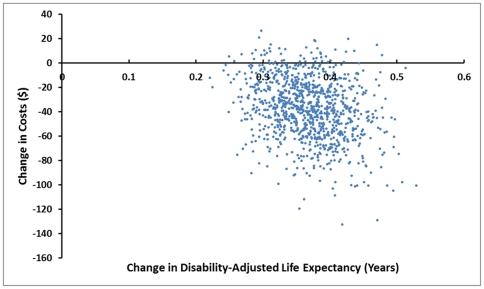
METHODOLOGY/PRINCIPAL FINDINGS: A Markov model was developed to compare the NCP to the status quo or current contraceptive program (CCP). The model followed a hypothetical cohort of 15-year old girls over a lifetime horizon. Data were obtained from the Uganda National Demographic and Health Survey and from published and unpublished sources. Costs, life expectancy, disability-adjusted life expectancy, pregnancies, fertility and incremental cost-effectiveness measured as cost per life-year (LY) gained, cost per disability-adjusted life-year (DALY) averted, cost per pregnancy averted and cost per unit of fertility reduction were calculated. Univariate and probabilistic sensitivity analyses were performed to examine the robustness of results. Mean discounted life expectancy and disability-adjusted life expectancy (DALE) were higher under the NCP vs. CCP (28.74 vs. 28.65 years and 27.38 vs. 27.01 respectively). Mean pregnancies and live births per woman were lower under the NCP (9.51 vs. 7.90 and 6.92 vs. 5.79 respectively). Mean lifetime societal costs per woman were lower for the NCP from the societal perspective ($1,949 vs. $1,987) and the MoH perspective ($636 vs. $685). In the incremental analysis, the NCP dominated the CCP, i.e. it was both less costly and more effective. The results were robust to univariate and probabilistic sensitivity analysis.
CONCLUSION/SIGNIFICANCE: Universal access to modern contraceptives in Uganda appears to be highly cost-effective. Increasing contraceptive coverage should be considered among Uganda's public health priorities.
在乌干达,超过三分之二需要避孕的女性无法获得现代有效的避孕方法。本研究旨在从社会和政府(卫生部)的角度,通过实施假设的新避孕方案(NCP),来估计在乌干达实现普及现代避孕药具的潜在成本效益。
方法/主要发现:建立了一个马尔可夫模型,将 NCP 与现状或现行避孕方案(CCP)进行比较。该模型对一组假设的 15 岁女孩进行了终生跟踪。数据来自乌干达全国人口与健康调查以及已发表和未发表的资料。成本、预期寿命、调整后残疾生命年、妊娠、生育率以及增量成本效益(以每获得一个生命年的成本、每避免一个调整后残疾生命年的成本、每避免一次妊娠的成本和每减少一个生育单位的成本来衡量)进行了计算。进行了单变量和概率敏感性分析,以检查结果的稳健性。NCP 方案下的预期寿命和调整后残疾生命年(DALE)的平均值高于 CCP(28.74 年对 28.65 年,27.38 年对 27.01 年)。NCP 方案下的每位女性的平均妊娠和活产数较低(9.51 次对 7.90 次,6.92 次对 5.79 次)。从社会角度来看,每位女性的终生社会成本 NCP 方案低于 CCP(1949 美元对 1987 美元),从卫生部角度来看,NCP 方案低于 CCP(636 美元对 685 美元)。在增量分析中,NCP 方案优于 CCP 方案,即成本更低,效果更好。结果在单变量和概率敏感性分析中具有稳健性。
结论/意义:在乌干达普及现代避孕药具似乎具有很高的成本效益。提高避孕覆盖率应被视为乌干达公共卫生的优先事项之一。